INTRODUCTION
Post-stroke dysphagia occurs in approximately 27%ŌĆō67% in acute stage [1,2]. Dysphagia is an important clinical problem because it causes serious sequelae, such as aspiration pneumonia and malnutrition, and reduces the quality of life [1,3]. Aspiration pneumonia is seven times more likely to develop in stroke patients with aspiration than in those without aspiration [4]. Post-stroke death is closely associated with aspiration pneumonia [5].
Various examination methods have been developed and used to evaluate swallowing function accurately, which is important in determining the proper treatment for patients [6]. Among these methods, the videofluoroscopic swallowing study (VFSS) is considered the gold standard [7,8].
A nasogastric tube (NGT) is easy to apply and relatively less invasive. Thus, it is commonly used to provide adequate nutrition to dysphagia patients [9]. However, prolonged NGT use can lead to complications, such as nasal wing lesions, chronic sinusitis, gastroesophageal reflux, and aspiration pneumonia [10]. These complications can worsen the patient's functional outcome. Therefore, appropriate and timely NGT removal in acute stroke patients with dysphagia is critically important.
To the best of our knowledge, no study has compared the occurrence of aspiration pneumonia after NGT removal alone and after NGT removal plus food thickening. Therefore, we aimed to investigate the safety of oral feeding with food thickener after NGT removal in acute stroke patients with thin liquid aspiration by evaluating the frequency of pneumonia in these patients.
MATERIALS AND METHODS
This retrospective study included acute stroke patients who presented to our rehabilitation unit between 2011 and 2015 for management of dysphagia. All patients had previously been assessed by neurologists and neurosurgeons when they were admitted to the acute stroke unit and underwent computed tomography (CT) or magnetic resonance imaging (MRI) to diagnose the stroke and determine the side, location, and size of the lesions. All patients who complained of symptoms of dysphagia were assessed by physiatrists and underwent VFSS. During hospitalization, patients underwent physical and occupational therapy as well as dysphagia therapy.
Criteria for patient selection were as follows: (1) first-time stroke confirmed by CT or MRI, (2) a history of NGT feeding due to dysphagia before VFSS, (3) VFSS within 3 weeks after stroke onset, (4) feeding method could be changed from NGT feeding to oral feeding after VFSS, and (5) no systemic infection present at the time of the VFSS. The exclusion criteria were as follows: (1) patients who could not undergo VFSS because of poor level of consciousness or who were unable to perform one-step obey-command, (2) who showed aspiration in examined materials except thin liquid, and (3) who had difficulties in the oral phase.
Patients were divided into two groups according to the severity of their dysphagia after VFSS. Patients who showed aspiration only with thin liquids were classified as group 1, and their feeding method was changed from NGT feeding to oral feeding with a food thickener (EasyMeal Toromi; Korean Drug Co. Ltd., Seoul, Korea) after VFSS. A food thickener was used to increase the viscosity of thin liquids (honey-thick liquids; viscosity >1,750 cP) to prevent thin liquid aspiration in group 1 [11,12]. Patients in group 2 showed no aspiration with thin or thick liquids, and their mode of feeding was changed from NGT feeding to oral feeding without a food thickener. All clinical examinations were performed and histories were obtained by physiatrists.
All patients underwent VFSS at approximately 2 weeks after stroke onset, and were monitored to identify the occurrence of aspiration pneumonia during the 4-week admission period. The present study was approved by the Institutional Review Board of Kyungpook National University College of Medicine (No. KNUMC_2016-03-024).
VFSS protocol
VFSS was conducted using fluoroscopy by an experienced physiatrist with radiologic technicians. A modified version of a previously published protocol was used [13]. The protocol consisted of two steps.
The first step was performed with fluoroscopy projected from the lateral side of the patient. Patients were first given a thick fluid bolus containing barium (3, 6, and 9 mL, with a viscosity of >1,750 cP), then a mechanically altered diet and regularly textured food, followed by a thin fluid bolus with barium (3, 6, and 9 mL, with viscosity of 1ŌĆō50 cP). Finally, two drinks of the thin fluid mixture were given with a cup [14]. The second step was performed as an anterior-posterior projection, with the patient sitting in an upright position. The patients were asked to drink 6-mL boluses of the thin-fluid mixture from a syringe.
In the event of high-volume aspiration, the study was aborted and the patients were encouraged to expectorate the food material. All food samples were administered twice. All the study procedures were recorded on AVI files (30 frames per second).
Measurements
The penetration-aspiration scale (PAS) was used for the quantitative evaluation of aspiration [15]. Numerical PAS scores were calculated using the physiologic parameters yielded by VFSS. The PAS scores were graded by the consensus of two physiatrists blinded to other clinical information.
Diagnosis of aspiration pneumonia after feeding change
All patients whose mode of feeding was changed from NGT feeding to oral feeding with (group 1) or without (group 2) food thickener after VFSS were monitored to identify the frequency of aspiration pneumonia during the admission period. After reviewing overall medical records, a diagnosis of pneumonia was made based on the following criteria: (1) the development of new radiographic infiltrate compatible with pneumonia, (2) the presence of symptoms or signs suggestive of lower respiratory tract infection (one major criterion of cough, sputum production, or temperature >38Ōäā or <35.5Ōäā and two minor criteria of pleuritic chest pain, dyspnea, delirium, increased alveolar arterial gradient, or white blood cell count >12,000/mm3 and/or left shift or leucopenia <3,000 mm3), and (3) the presence of risk factors for oropharyngeal aspiration [16].
Statistical analysis
All statistical analyses were performed using PASW Statistics ver. 18 for Windows software (SPSS Inc., Chicago, IL, USA). Student t-tests were conducted to assess the significance of difference between the PAS scores of groups 1 and 2, and the Žć2 test was used to compare the incidence rate of aspiration pneumonia between groups 1 and 2. A p-value<0.05 was considered statistically significant. The intra-class correlation coefficient (ICC) model of the PAS was calculated to test inter-rater reliability. An ICC value >0.80 was considered very good, 0.61ŌĆō0.80 good, 0.41ŌĆō0.60 moderate, 0.21ŌĆō0.40 fair, and <0.21 poor [17]. The consistency of other items was evaluated using Cohen's kappa.
RESULTS
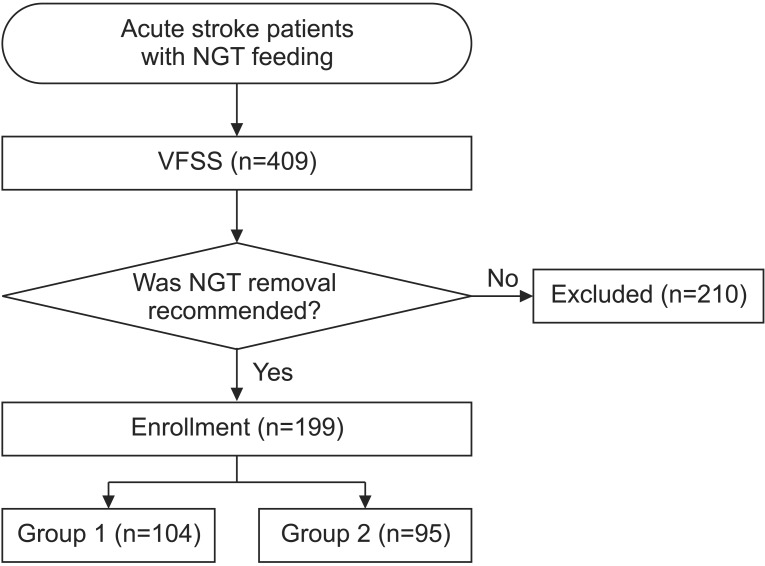
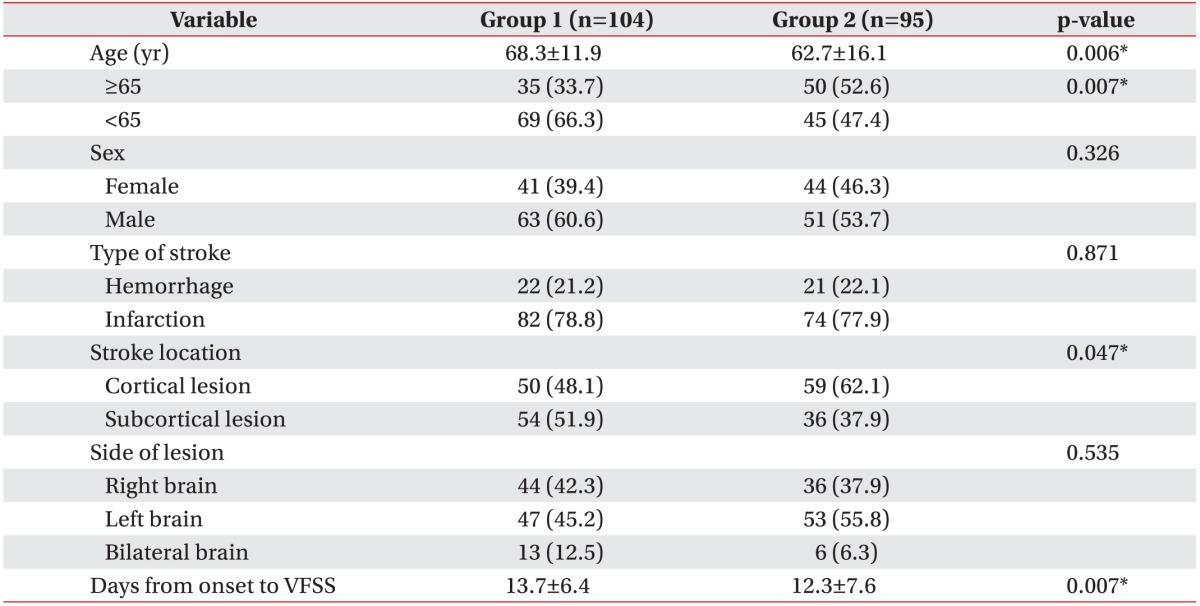
A total of 409 patients with NGT feeding underwent VFSS. A total of 199 (33.4%) dysphagic patients were included in the study: group 1, 104 patients; group 2, 95 patients (Fig. 1). In group 1, 40 patients were changed from NGT feeding to a regular diet and 64 patients were changed to dysphagia diet levels as follows: level 1 (15 patients), level 2 (24 patients), and level 3 (25 patients) after VFSS. All 95 patients in group 2 were changed from NGT feeding to a regular diet. Infarction was the most common lesion in both groups. Other demographic characteristics are listed in Table 1.
The ICC between the two physiatrists was good, and a similar result was found between the PAS scores of groups 1 and 2 for the thick and thin liquid examination in VFSS (ICC=0.851 and 0.806, respectively). The PAS scores for thick and thin liquids were 1.92┬▒0.73 and 6.46┬▒0.65, respectively, in group 1, and 1.53┬▒0.58 and 2.65┬▒0.74, respectively, in group 2 (Table 2). There was a significant difference in PAS scores for thin liquids between groups 1 and 2 (p<0.001).
Aspiration pneumonia was identified in 1.9% (2/104) of group 1 and in 3.2% (3/95) of group 2. Oral feeding was stopped in patients with aspiration pneumonia, and the NGT was reinserted. After reinserting the NGT, there was no recurrence of pneumonia. The incidence rate of the aspiration pneumonia between the groups showed no significant difference (p=0.578) (Table 3).
DISCUSSION
This study has shown that NGT removal together with the use of a food thickener in acute phase with thin liquid aspiration does not increase the incidence of aspiration pneumonia after stroke; thus, diet modification with the use of a food thickener can be recommended.
Previous studies reported that pneumonia occurred in 5.6% of patients [18] and in 5.9% of stroke patients admitted to a rehabilitation unit [19]. The present study showed a lower occurrence of aspiration pneumonia than other studies. One reason is the mild degree of dysphagia in our participants. Another reason is that the 4-week follow-up after VFSS was not long enough to identify the occurrence of aspiration pneumonia.
The current recommendation for the management of swallowing in dysphagic patients is based on the prevention of aspiration such as swallowing maneuvers, volume control, dietary changes, and NGT use [20,21]. Stroke patients with dysphagia have more difficulties swallowing fluids than solid food [14]. This is probably because of the difficulty in controlling a thin bolus and/or the delayed or absent trigger of the swallow reflex. Abnormal swallowing due to impaired coordination, obstruction, or weakness affecting swallowing biomechanics can cause aspiration and have been found to be important risk factors for stroke-associated pneumonia across different clinical studies [22,23,24]. Thus, NGT feeding is commonly used to provide adequate nutrition to acute stroke patients with dysphagia rather than swallowing maneuvers [9].
However, prolonged NGT insertion may cause various complications, such as nasal wing lesions, chronic sinusitis, gastroesophageal reflux, and aspiration pneumonia [12]. Furthermore, one study reported an important negative impact of NGT use on the quality of life because eating is considered not only a vital function but also a daily pleasurable activity and social tradition [25]. Although a patient using NGT feeding is nourished, the meal is limited to its functional role; its social role disappears, and the patient no longer derives pleasure from it. In addition, NGT feeding can induce discomfort, which is also a reason for the change in body image. Therefore, one can speculate that these modifications interfere with the patient's quality of life [26,27]. Thus, if no evidence of aspiration is found on VFSS, immediate removal of the NGT is recommended. Furthermore, patients who have thin liquid aspiration on VFSS can change from NGT feeding to oral feeding using a food thickener. The efficacy of using a food thickener, despite weak oropharyngeal swallowing, is derived from a prolonged pharyngeal transit duration [28] due to the slowed flow characteristics inherent in a thickened liquid bolus [29] that prevent the bolus from being aspirated, thereby allowing for a successful swallow.
Dysphagia is defined as a difficulty in the oral, pharyngeal, or combined oral-pharyngeal phases of swallowing [30]. In the oral stage, patients with oral phase dysfunction have difficulty with bolus control, and may attempt to swallow incompletely masticated food. Factors that increase the bacterial load and the risk of oral colonization due to potentially pathogenic organisms may increase the risk of aspiration pneumonia [31]. Pharyngeal phase dysphagia with residue, inhalation of food after swallowing, or inadequate closure of the airway, is expected to be associated with an increased incidence of aspiration pneumonia [32,33]. In this study, patients who had difficulties with the oral phase were excluded; therefore, aspiration pneumonia due to oral phase problems was not considered.
This study had several limitations. First, regarding subject selection, patients who had a certain degree of swallowing function and did not have definite oral phase difficulties were included in our study. Second, 4-week follow-up after VFSS was not long enough to identify the occurrence of aspiration pneumonia. Third, we used only one brand of food thickener, which was not representative of other food thickeners. Fourth, we could not exclude significant differences in the characteristics of groups 1 and 2 (age, stroke lesion, and days from onset to VFSS).
In conclusion, this study showed that changing acute stroke patients presenting thin liquid aspiration from NGT feeding to oral feeding with a food thickener does not lead to a higher occurrence of aspiration pneumonia, compared with acute stroke patients without thin liquid aspiration. Therefore, we recommend prompt VFSS in acute stroke patients suspected of having thin liquid aspiration to avoid unnecessary and prolonged NGT use.