INTRODUCTION
Spinal cord injury (SCI) is a devastating condition that often results in significant physical, psychological, and social consequences for affected individuals, potentially leading to even more serious outcomes such as suicide [1,2]. Understanding suicidality in the SCI population is of utmost importance, as individuals with SCI reportedly have more than a three-fold higher suicide incidence than those without SCI [3,4]. It has also been observed that 34.8% of individuals with chronic SCI experience suicidal ideation, with 17.3% having attempted suicide and a maximum of 11% resulting in fatalities [5].
Several studies have been conducted to elucidate risk factors for suicidality in patients with SCI [6-11]. Various psychological components, including a history of suicide attempts, depression, impulsivity, self-esteem issues, and alcohol misuse, have been recognized as significant contributors to suicide risk in individuals with SCI [6,8]. Social disconnection, such as unemployment, has also been associated with increased suicidality [7,12].
While many studies have focused on the direct impact of mental and social aspects on SCI suicidality, there remains a relative lack of understanding regarding connections between the suicide tendencies of the SCI population and their physical and functional characteristics [9-11,13,14]. A fundamental consideration for the SCI population is that SCI primarily results in physical and functional challenges for affected individuals [15-17], in addition to psychosocial issues. While it is recognized that physical conditions like spasticity, pain, or reduced mobility often lead to greater dependency in daily activities and a diminished quality of life and self-identity [18-21], few studies have explicitly examined the impact of these physical and functional constraints on suicide risk [10,13]. Therefore, to identify those most at risk of suicide within the SCI population, it is important to understand how physical discomfort or functional dependency in SCI relates to suicide risk.
This study aimed to explore how certain physical and functional characteristics of individuals with SCI might correlate with reported suicidality. By understanding the combined psychosocial and physical risk factors for suicide, we aim to offer comprehensive prevention measures and early interventions for the SCI population.
METHODS
Participants
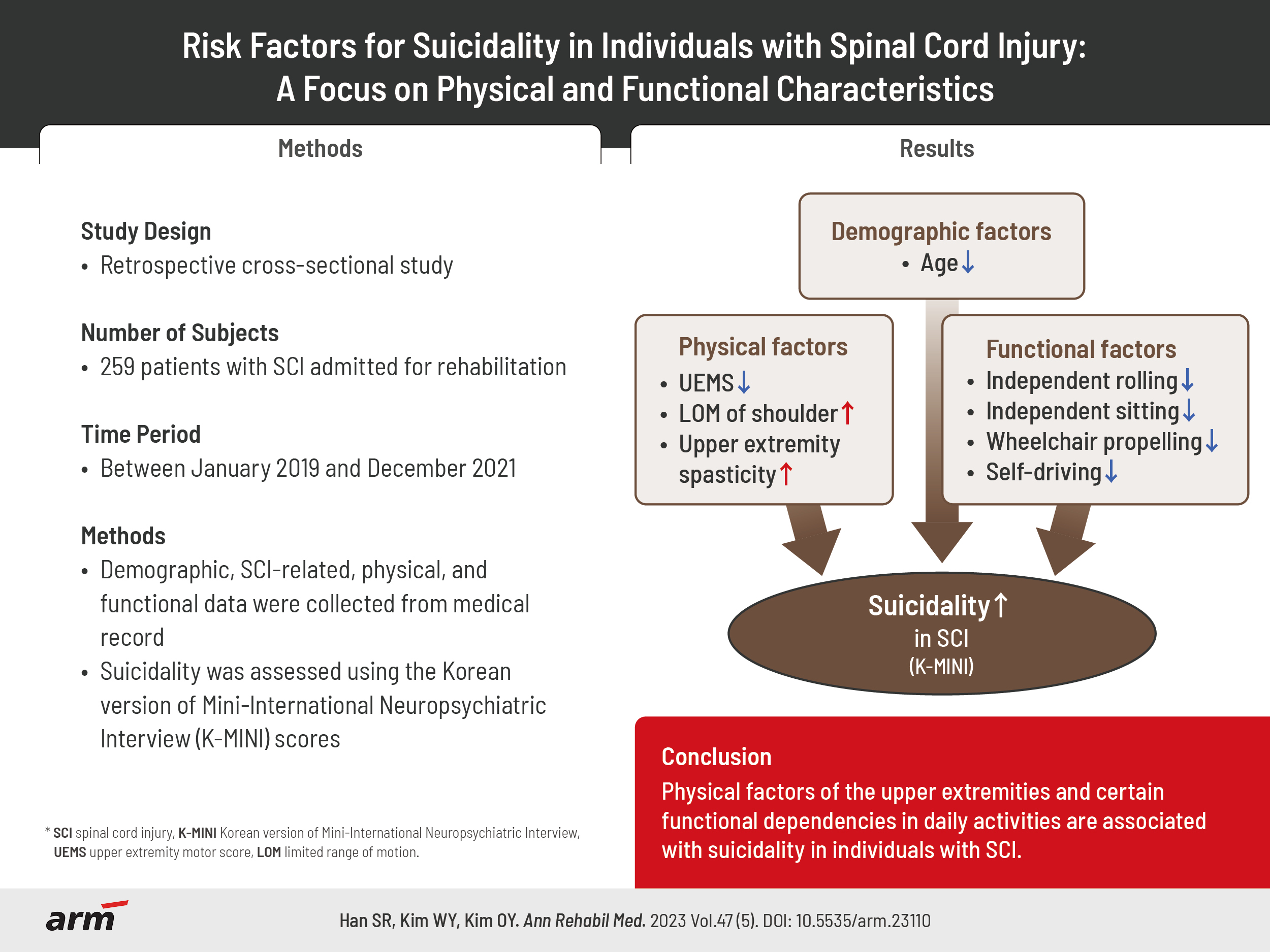
In this retrospective, cross-sectional study, the medical records of inpatients with SCI admitted to the SCI unit at the National Rehabilitation Center, Seoul, Korea, between January 2019 and December 2021 were assessed. The inclusion criteria for psychological evaluation encompassed individuals who were 18 years of age or older, possessed the capability of engaging in normal communication, and demonstrated the ability to understand and complete the survey. Individuals who did not understand the survey content or did not wish to participate were excluded. All psychological evaluations were conducted after obtaining informed consent from the participants. Among the 411 inpatients during the research period, 259 who underwent psychological evaluation were identified. This study was approved by the Institutional Review Board of the National Rehabilitation Center (#NRC-2022-01-005).
Data collection
Data collected included demographic factors (age, sex, body mass index, educational level, and current occupation) and SCI-related factors (duration from injury onset, severity of SCI or completeness of injury, neurological level of injury [NLI], and etiology of injury) from admission medical charts. Physical characteristics (upper extremity motor score [UEMS], lower extremity motor scores, limited range of motion [LOM] of the shoulder and hip, and spasticity of the upper and lower extremities) and functional characteristics (dependency on rolling, coming to sit, wheelchair propelling, functional ambulation categories scales, and capability of self-driving) were extracted from the physical therapy evaluation reports performed at the time of admission. These variables were classified into four groups (demographic, SCI-related, physical, and functional) based on each characteristic.
Measurement of suicidality
The assessment of suicidality was performed within one week from the date of admission. A psychologist with more than 10 years of clinical experience evaluated participants’ suicidality using the Korean version of the Mini International Neuropsychiatric Interview (K-MINI) [22]. The K-MINI module comprises six questions: wish for death (1 point), wish for self-harm (2 points), suicidal thoughts (6 points), suicide plans (10 points), suicide attempts in the past month (10 points), and lifetime suicide attempts (4 points) [23]. The total K-MINI score was calculated from the sum of the six questions, and the severity of suicidality was determined. Those with a score of 5 or below indicated a low suicide risk group and those with a score of 6 or above indicated a high suicide risk group. Psychological counseling has been recommended for individuals in the high suicide risk group.
Statistical analysis
All the statistical analysis were performed using IBM SPSS Statistics 27.0 (IBM Corp.). Participant characteristics were presented as mean±standard deviation for continuous variables, and numerical values (n) and percentages (%) for categorical variables. The association between the variables (demographic, SCI-related, physical, and functional characteristics) and suicide risk was evaluated using an independent t-test for categorical data and a Pearson correlation test for numerical data. To examine the risk factors for suicidality, simple and multiple linear regression analysis were performed using K-MINI suicide scores as the dependent variable. Beta (β) was used to represent the change in the dependent variable for each unit change in the independent variable. Statistical significance was set at p<0.05.
RESULTS
Table 1 shows the demographic and clinical characteristics of participants. The average age of the 259 participants was 49.1±16.5 years, and 196 were male (75.7%). Of the total sample, 150 (63.8%) were unemployed. Regarding SCI-related factors, the average duration since injury was 716.7±1,867.8 days. According to the American Spinal Injury Association classification [24], incomplete injuries were more prevalent (68.1%). Tetraplegia and paraplegia accounted for 55.1% (n=140) and 44.9% (n=114) of the cases, respectively. A total of 177 (70.2%) individuals had traumatic SCI. The UEMS group obtained an average score of 35.9±15.7. Among the physical values, 35.7% (n=91) of the study participants reported LOM of the shoulder and 28.2% (n=72) had upper extremity spasticity. Suicidality, as assessed by the K-MINI module, had an average score of 1.8±3.3.
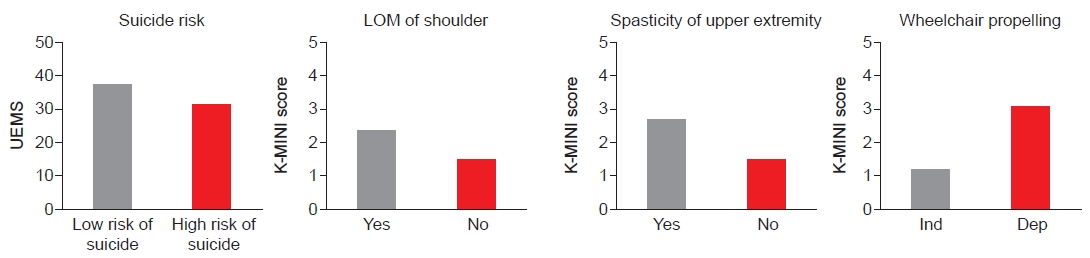
When analyzing the association between associated factors and suicide risk (Table 2), age showed a statistically significant negative correlation with suicidality (r=-0.162, p=0.021). However, no significant correlations were observed with sex, education, or occupation. Regarding SCI-related factors, no statistical significance was found in terms of the duration of injury, completeness, NLI, injury etiology, or their relationships with suicidality (p>0.05). Regarding physical characteristics, a statistically significant negative correlation was observed between UEMS and suicidality (r=-0.144, p=0.042). Compared to the low risk group, the average UEMS in the high suicide risk group was 6.5 points lower (p=0.037) (Fig. 1). Although the average total K-MINI scores were respectively 0.9 and 1.2 points higher in individuals with LOM of the shoulder (p=0.070) and upper extremity spasticity (p=0.028), no statistically significant relationships were found between the presence of all types of LOM or spasticity and increased suicidality. Among the functional characteristics, a significantly higher suicide risk was observed in cases in which participants were incapable of performing independent rolling (p=0.014), sitting (p=0.018), and wheelchair propelling (p=0.004). In particular, the average total K-MINI score of the dependent wheelchair propellers was 1.86 points higher compared to that of the independent group (p<0.001). There was also significantly higher suicidality among participants unable to drive compared to those capable of self-driving (p=0.001).
In the simple linear regression analysis examining the factors influencing suicide risk, as measured by the total K-MINI scores (Table 3), the following predictors were identified as statistically significant: age (β=-0.16, p=0.021), UEMS (β=-0.14, p=0.042), spasticity of the upper extremity (β=0.16, p=0.028), dependency of rolling (β=-0.20, p=0.005), come to sit (β=-0.17, p=0.016), and wheelchair propelling (β=-0.26, p<0.001).
A multiple linear regression analysis revealed that among the physical factors, lower UEMS (β=-0.63, p=0.027), shoulder LOM (β=0.33, p=0.031), and upper extremity spasticity (β=0.47, p=0.023) were significant predictors of increased suicide risk. Among the functional characteristics, independent wheelchair propelling was a predictor of lower suicide risk (β=-0.43, p=0.018; Table 4).
DISCUSSION
In this study, we analyzed the association between the demographic, SCI-related, physical, and functional characteristics of participants with SCI and their suicidality based on total K-MINI scores. Results indicated that age had a statistically significant negative correlation with suicide risk. No significant associations were found with SCI-related factors, including duration from injury, completeness, and NLI. Among the physical characteristics, UEMS was significantly associated with higher suicidality scores, and lower UEMS was found to be a predictor of increased suicide risk. In terms of functional characteristics, the inability to perform independent rolling, sitting, wheelchair propelling, and self-driving was associated with higher suicidality. Specifically, independent wheelchair propulsion was a predictor of lower suicide risk. The analysis also indicated that LOM of the shoulder and upper extremity spasticity were predictors of higher suicide risk.
Overall, the most notable study findings pertain to the physical and functional characteristics of suicidality. With regard to physical characteristics, a lower UEMS score was found to be a predictor of increased suicide risk. Considering that UEMS is an indicator of functional dependency in SCI [25] and that muscle strength plays a key role in independent self-care in individuals with SCI [26], study participants with lower UEMS scores were presumed to have struggled to pursue functional day-to-day lives. These dependencies could lead to diminished self-efficacy and desire for life [16,27,28]. Moreover, in the current study, LOM of the shoulder and upper extremity spasticity were identified as predictors of higher suicide risk. Together with the lack of muscle strength, these physical discomforts could have concurrently contributed to the participants’ mental health deterioration by causing a range of functional disturbances [15,29-31]. Physical discomfort in the lower extremities was not of particular significance. A pilot study revealed that joint contractures, particularly in the upper extremities, can negatively affect functional abilities in individuals with SCI [29]. Similar to the associations observed with physical characteristics, our results on functional characteristics provided significant insights, especially with wheelchair propulsion, a functional movement performed using the upper extremities [15]. Overall, our findings underscored the need for appropriate interventional strategies for patients with SCI with physical and functional concerns, particularly in the upper extremities.
Interestingly, among the SCI-related factors, NLI and completeness did not demonstrate any significant associations with suicidality. Previously, some studies focused on the relationship between actual death by suicide and SCI-related characteristics. Prior investigations have reported the highest standardized mortality ratio in patients with complete paraplegic SCI [4,32] and recommended caution to prevent suicide in individuals with SCI and complete injury [10]. Other reports have presented a nearly two-fold higher suicide mortality rate in paraplegic SCI than in tetraplegic SCI [7,11]. However, as these earlier findings are refined to the actual mortality of suicide, further investigation is warranted to determine the tangible impact of completeness or the level of injury on overall suicidality in the SCI population.
A meaningful correlation among demographic factors was observed between age and suicidality. This result aligns with the outcomes of previous studies that demonstrated the vulnerability of the younger population with SCI to suicide [10,33]. Before injury, young individuals often maintain a higher level of physical activity and social interaction than older adults, which may lead to a relatively greater sense of impairment and discouragement [12,34]. However, in this study, occupation did not show any statistically significant correlations with suicidality. This result was inconsistent with findings from the general population [35]. It is important to note that the study participants reported their current employment status while they were hospitalized or on leave. As a significant number of SCI populations struggle against the uncertainties of returning to their prior occupations [36,37], reliable analysis should be conducted within social backgrounds.
The present study had several limitations. Owing to the retrospective cross-sectional study design, the establishment of a cause-and-effect relationship was challenging. Additionally, the single-center recruitment of participants and sole inclusion of inpatients with SCI jointly restrict the generalizability of the findings. Our study also lacked information about the participants’ specific occupations, economic status, and information regarding their caregivers, whether paid or family. Lastly, as the analysis of suicidality was based on the total K-MINI score to reflect overall suicidal tendencies, the results should be applied with caution when it comes to capturing the nuances of individual elements such as suicidal thoughts, suicide plans, and suicide attempts.
Understanding physical and functional suicide risk factors in populations with SCI is essential for several reasons. It provides support for identifying high risk individuals for targeted interventions and informs the development of tailored rehabilitation programs. Our study demonstrated that physical factors of the upper extremities and certain functional dependencies in daily activities are associated with suicidality in individuals with SCI. Considering this, our findings can contribute to the advancement of early intervention strategies for suicide prevention in individuals with SCI. This can be achieved by highlighting the necessity for structured physical and functional rehabilitation programs that incorporate upper extremity training and wheelchair activities.