INTRODUCTION
Cardiac rehabilitation (CR) is an essential component in the continuum of care for patients with cardiovascular disease. The safety and efficacy of CR are well documented, but CR participation rates remain low and suboptimal worldwide. Despite being eligible candidates, over 80% of patients in the United States and 50% in the United Kingdom do not participate in CR [1,2]. Factors such as reluctance to participate in group rehabilitation, inconvenient exercise schedule, career responsibilities, transportation, and related costs were prominent barriers to CR participation [3,4]. In addition, during the coronavirus disease 2019 pandemic, safe distancing measures have led to cessation of center based cardiac rehabilitation (CBCR) programs [4].
Home based cardiac rehabilitation (HBCR) has been introduced as an alternative strategy to expand access and participation over conventional CBCR [3,5]. In concept, HBCR could help overcome barriers for CBCR such as geographic, occupational and other access related barriers.
Heart rate (HR) is an important parameter for determining appropriate exercise intensity and establishing a safe zone when performing self-monitored aerobic exercise during HBCR [6,7]. Commonly, patients are instructed to take pulse rate (PR) at their radial or carotid artery and measure their arterial beats for 10 seconds (and multiply it with 6 to get HR per minute), but this method is difficult and inconvenient during aerobic exercise and also is less accurate [6].
With the recent development of technology, commercial electronic devices with HR monitor in forms of chest straps, smart watches and smart bands have been introduced and are being used worldwide. The HR measurement derived from these tools not only reflect patient’s condition but also provides guidance for appropriate exercise [7].
Researches on the accuracy and validity of HR measuring wearable devices have been actively reported [6-13]. However, the reports on HR accuracy so far are somewhat inconsistent. Depending on type of the devices, such as chest strap, patch, smart band or smart watch, the HR accuracy was variable. Chest strap type tended to be more accurate than other wrist worn devices [8]. Smart watches were more accurate in terms of HR (actually PR) than relatively inexpensive smart bands [8-10]. Also, the accuracy of these devices fluctuated in accordance to the intensity or type of exercise [6,10]. HR measured by smart band seemed to be inaccurate with high intensity aerobic exercises [6].
To the best of our knowledge, although previous reports were made recently, these studies were conducted with relatively old and inexpensive series of available wearable devices [7,8-13]. In this study, we used the latest products from the two electronics companies with the largest market share in the world, which are Apple watch 7 (AW7; Apple Inc.) and Galaxy watch 4 (GW4; Samsung). We also included a recently introduced patch type HR monitoring device, Bio Patch Mobicare 200 (MC200; Seers Technology), to compare with the smart watches.
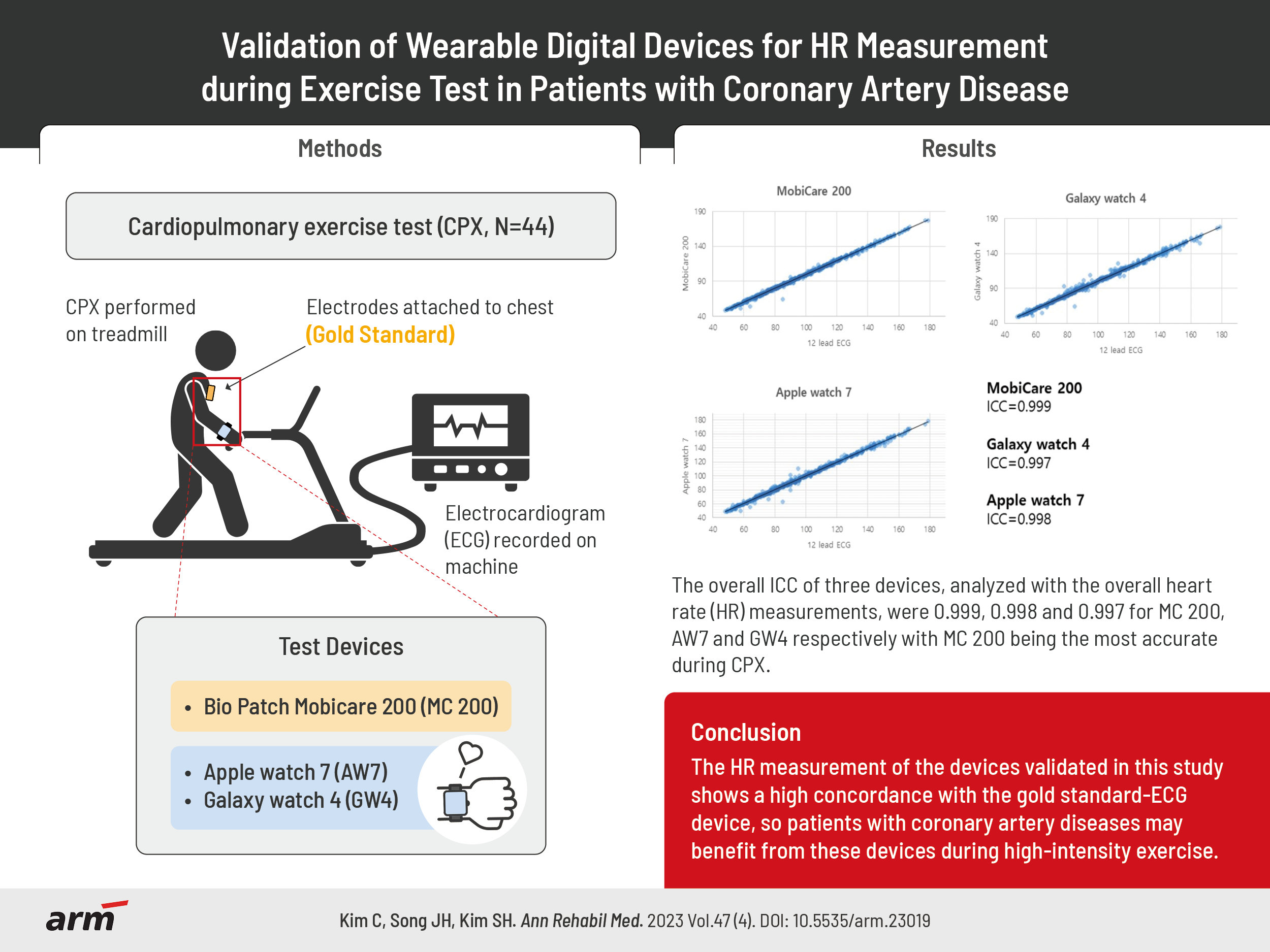
We hypothesized that the newer wearable devices compared to the older models would be more accurate with HR monitoring and show higher correlation with the 12 lead electrocardiograph (ECG), which is the gold standard. This study aimed to confirm the validity and accuracy of HR measurement in recently released commercial smart watches and chest patch device, during cardiopulmonary exercise test (CPX).
METHODS
The study protocol was approved by the Institutional Review Board of Inje University (no. 2021-10-007). All the participants provided written informed consent. The researcher explained the purpose, methods, advantages, and potential risk of the study to every participants. Patient privacy and data confidentiality were maintained throughout the study period. The smart watches used in the study were purchased at researcher’s own expense. The authors declare no conflict of interest.
Sample size calculation
Since free software calculating sample sizes for reliability coefficients are relatively scarce, the calculation was performed on a web-based calculator in accordance to the article by Arifin [14]. The test-retest reliability of a measurement tool by intraclass correlation coefficient (ICC) is expected=0.9. The measurement was taken at two occasions (12 lead ECG vs. each wearable device). The lowest acceptable ICC is 0.75 [14,15]. A significance level of α=0.05 and a power of 90% were set. In conclusion, 44 subjects were required for this study.
Participants
This was a comparative observational study recruiting outpatients of Cardiac Rehabilitation Clinic at Inje University Sanggye Paik Hospital, Inje University College of Medicine, from June 2022 to September 2022. We included 44 patients aged 20 to under 75, diagnosed with coronary artery disease, including acute coronary syndrome and stable angina, and subsequently referred for CR. These patients were scheduled for outpatient CPX as a regular follow-up exam. For this study, the participants had to put on extra wearable devices while going through CPX. Patients with contraindications to CPX were excluded according to the guideline by the American Heart Association (AHA) [16]. Also, patients referred for CR with other cardiac etiologies, such as valvular or aortic disease, were excluded from the study.
CPX
CPX was performed on a treadmill and stress test system (T-2100 & CASE; GE Healthcare) according to the modified Bruce protocol. In this study, respiratory gas analyzer (Quark CPET; COSMED), automatic blood pressure and pulse monitor (TANGO M2; SunTech) were used to measure physiologic variables. The HR recorded from the CPX machine was set as the gold standard.
All three wearable devices used in this study were recently released products within a year. MC200 is a device approved for long term ECG recording by the Korean Ministry of Health and Welfare in February 2022. MC200 was attached along the axis of lead II, from lateral aspect of left upper sternum to apex of heart. GW4 and AW7, which are wrist strap type, were worn around left and right wrists respectively. We looked up in the product instructions and fitted the watches exactly where it should be (2–3 cm above styloid process of radius). It was fixed to a hole of a strap that could fit the device as tight as we could so it doesn’t move sideways, but also not as much as it would choke patient’s wrist. To reduce the bias caused while fastening the strap, one researcher helped put on the device in person so that the straps were adjusted to participants’ wrist with less inconsistency.
In the rest phase, which lasted for 6 minutes, patients were sat on a chair while blood pressure and ECG were being monitored. HR from 12 lead ECG and wearable devices were recorded every two minutes during the rest phase. After 6 minutes, exercise phase started according to the modified Bruce protocol with gradual increase in intensity and HR was recorded every minute during all exercise stages until termination of the test. The participants held handrails in front of them to prevent serious harm during the CPX test since the most participants were middle-aged. Termination of the test was decided according to the “Indications for termination of exercise testing” of AHA guidelines [16]. Lastly, in the recovery phase, patients kept walking slowly for additional 5 minutes, and HR was measured every minute (Fig. 1).
Statistical analysis
All data were analyzed using IBM SPSS ver. 25 (IBM Corp.) and the values were presented as means±standard deviation (SD) or numbers and percentages. The HR data from gold standard 12 lead ECG and each wearable devices were analyzed with following parameters.
First, paired relative difference and paired absolute difference (PAD) were calculated to assess accuracy, by subtracting the HR recorded by wearable devices (HRDEV) from the HR recorded by the 12 lead ECG from CPX machine (HRECG). Also, mean absolute percentage error (MAPE) values were calculated as the average absolute value of the errors of each wearable device relative to 12 lead ECG, the gold standard measure, expressed in percentage. Fokkema et al. [17] suggest a MAPE threshold of 5%, whereas Nelson and Allen [18] used a MAPE threshold of 10% to classify a wearable device as valid.
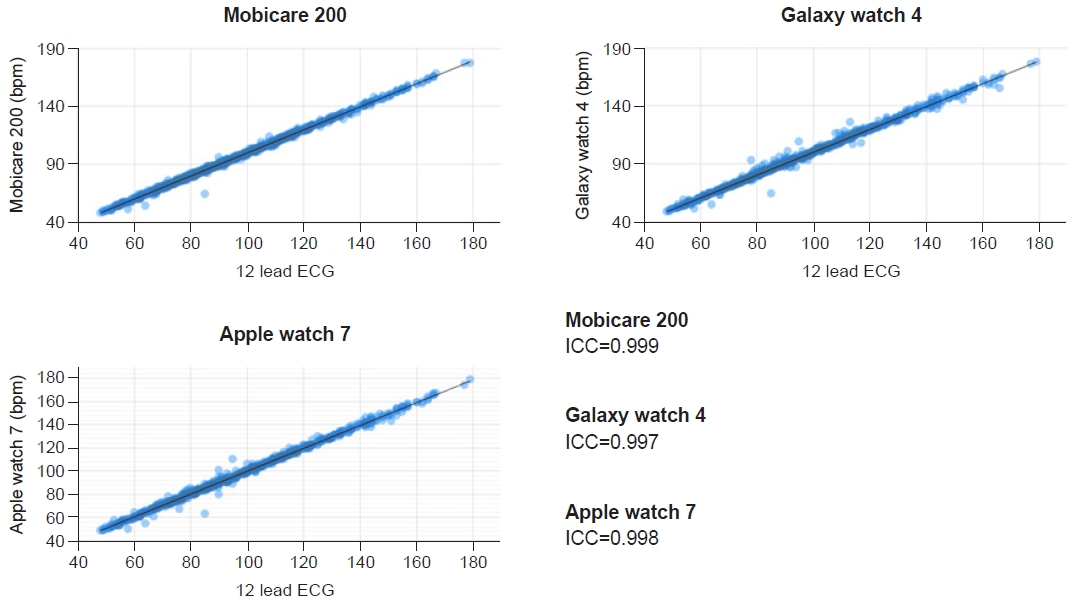
The degree of agreement between the values of two devices was examined using the ICC with 95% confidence interval (CI). The thresholds suggested by Fokkema et al. [17] were used; excellent, 0.90 or above; good, 0.75–0.90; moderate, 0.60–0.75; and low, 0.60 or below.
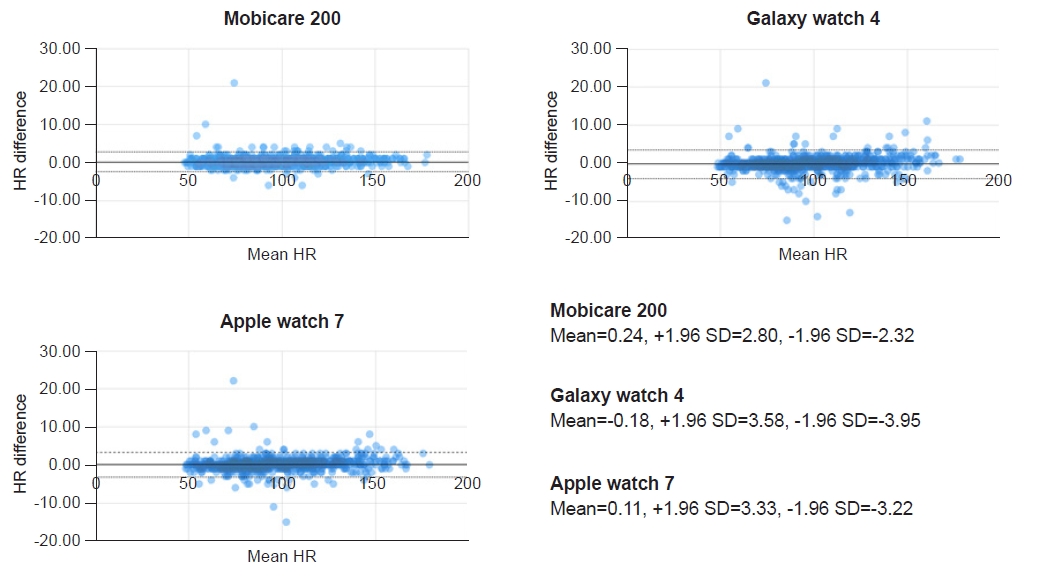
In addition, Bland–Altman plot with 95% limits of agreement (LoA) was used to measure each outcome relative to the gold standard. The differences of each sample are scattered on the vertical axis and the average of two measurements are scattered on the horizontal axis. The plot contains three horizontal lines indicating the mean difference and upper and lower LoA which could be calculated as the mean difference±1.96 SD of differences [19].
RESULTS
Total 44 of 36 male and 8 female patients were included for the study. In CPX results, average attained stage was 6.0, lasting average 16 minutes 26 seconds. Average rate of perceived exertion was 16.4 with respiratory exchange ratio of 1.2. The average of peak oxygen uptake and peak metabolic equivalents were 25.8 and 7.4, respectively. The baseline characteristics and summary of CPX results are presented in Table 1. Incidence of arrhythmias during CPX test and total number of HR records for each patient are described in Table 2. There were participants with frequent premature beats but there were no sustained arrhythmias that could fluctuate HR during CPX.
Average paired relative difference and relative percent difference of all the devices were within absolute value of 1 at all phases (Table 3). Average PAD were also around 1 at all phases, with AW7 showing maximal 1.29 at recovery phase. Absolute percent difference of all three devices at all phases did not exceed value of 2%. ICC of all the devices exceeded 0.99 at all the phases, except for AW7 resulting in 0.984 at rest phase but still showing excellent correlation.
On the other hand, influence of HR itself on accuracy of the devices were evaluated. HR recordings from exercise phase and recovery phase were grouped into two subgroups of “HR below 100” and tachycardia, which were “HR at or above 100” (Table 4). PAD, MAPE, and ICC were obtained. Although not always statistically significant, there were some tendency of HR accuracy variability according to HR and CPX phases. PAD values tended to be larger when HR was above 100, and MAPE values tended to be larger when HR was below 100. However, PAD and MAPE did not exceed value of 2 and ICC values were above 0.9 in every circumstances regardless of HR or phases.
Fig. 2 presents Bland–Altman analysis, where solid horizontal lines indicate the average HR differences in each device. Two dashed lines indicate upper and lower 95% confidence LoA for each device respectively. MC200 showed average difference of 0.24, with upper and lower LoA of 2.80 and -2.32, respectively. Average difference of GW4 was -0.18 with 95% LoA of 3.58 and -3.95. Lastly, AW7 had mean value of 0.11 and 95% LoA of 3.33 and -3.22, respectively.
In Table 5, ICC values of the devices in accordance to HR divided into interval of 20, ranging from below 100, 100–119, 120–139, 140–159 to at or above 160 were analyzed. The ICC value was highest at HR below 100 in all three devices. The accuracy decreased when HR was over 100 in all groups. GW4 showed the lowest ICC of 0.867 at HR at or above 160 and AW7 showed the lowest value of 0.925 at HR between 140–159. MC200, on the other hand, showed minimum ICC of 0.980 at HR between 100–119 and 120–139.
The overall ICC of three devices, analyzed with the overall HR measurements, were 0.999, 0.998, and 0.997 for MC200, AW7 and GW4 respectively with MC200 being the most accurate (Fig. 3).
DISCUSSION
In this study, we aimed to verify the accuracy of HR monitoring function of wearable devices by performing the CPX according to the modified Bruce protocol. The devices used in the study, all commercialized recently, were AW7 and GW4, both of which were released by the top 2 largest electronics companies in the global smart watch market. For comparison, MC200, a chest patch type device for a long-term ECG recording approved by the Korean Ministry of Health and Welfare on February 2022, was adopted.
A few earlier studies have assessed the HR accuracy of various smart devices. Boudreaux et al. [9] reported the average MAPE of Apple watch 2 as 4.14 and the average ICC as 0.9. But, the exercise intensity was reported to affect the HR accuracy with the MAPE as 7.16 at maximum at high intensity exercise and the ICC as 0.8 at minimum [9]. In another study, the values of the MAPE were all affected by the exercise intensity. The MAPE of Apple watch (series unclarified) varied from 1.14% to 6.70%—the highest MAPE value in the moderate intensity exercise; the MAPE of Fitbit from 2.38% to 16.99%; and the MAPE of Garmin Forerunner 225 from 7.87% to 24.38% [10]. Likewise, the overall HR accuracy depended on the type of devices, series, and models, and the type of exercise and intensity.
Many other studies have showed somewhat high MAPE and low correlation coefficient value with less accurate HR values of the devices during exercise [7,8-13]. Though chest-patch devices are known to be more accurate than other types of devices, it was reported that even the chest-patch devices (Mobicare 100) showed a correlation coefficient of 0.69 during high intensity exercise with above HR 160 [6,8].
In contrast, the devices used in this study showed the MAPE value of less than 2% and ICC value of over 0.9 in every circumstance, which shows a high correlation with the gold standard 12 lead ECG—except the HR measurement from GW4 in high intensity exercise phase with HR over 160, showing ICC of 0.867. Still, the minimum value of ICC still showed a good correlation that is similar or higher than that of previous reports conducted with other older devices.
In the exercise phase of modified Bruce protocol, the exercise intensity increases every three minutes. Also, when the CPX terminates, the exercise intensity and the HR begins to decrease radically in recovery phase. The initial increase of HR in the exercise phase are caused by the parasympathetic withdrawal, while sympathetic activation is responsible for HRs greater than 100 beats/minute. Also, the rapid drop in HR for the first minute after the cessation of exercise is mostly determined by parasympathetic reactivation [20]. Due to the impaired autonomic regulation, CAD patients show delayed HR recovery which may take up to five minutes [21,22]. We postulated that such changes in HR according to the exercise intensity would affect HR accuracy of the devices.
Accordingly, the HR measurements in the exercise and recovery phase were divided into four subgroups based on “HR below 100” and “HR above 100.” Since the MAPE is an indicator expressed as percentage, the MAPE values tended to be small when the denominator was greater than 100, and be big when the denominator was less than 100 (Table 4). Thus, the PAD was analyzed along with the MAPE for precise comparison.
The PAD values of MC200 and AW7 were significantly larger in recovery phase than in exercise phase. The PAD values of GW4 and MAPE values of all the devices did not show any significant difference between phases, but the values tended to be larger in recovery phase than those in exercise phrase as postulated. However, since the HR difference between phases were about 1 bpm on average, the difference would not indicate any clinical significance in the real world. Also, ICC values exceeded 0.9 in all conditions, which showed a high reliability. In addition, the comparison between the HR subgroups within the same phases showed some significant differences, but the results were inconsistent.
To examine HR accuracy in accordance with the exercise intensity, we stratified the HR measurements by the interval of 20. As in Table 5, the ICC of all three devices were highest when HR was below 100. Though the ICC tended to decrease as HR increased, the relationship was not linear, in that it showed the lowest ICC at the moderate intensity of HR between 140 and 159 in MC200 and AW7. It is consistent with the previous studies that suggest a higher accuracy with vigorous exercise than with slow walking [23-25]. However, as previously mentioned, the lowest ICC values of all three devices were still higher than those of other studies, indicating an overall high level of accuracy regardless of the exercise intensity.
As chest-strap-based HR monitors were first introduced in the 1980s, several studies have already confirmed the accuracy of these monitors as a prototype of HR measuring devices [26-28]. However, these devices were only used by elite athletes due to its inconvenience. Nowadays, new, convenient wrist-worn HR monitors have garnered public attention. Unlike the chest-strap type directly sensing one’s cardiac electric activity, these devices use photoplethysmogram (PPG) sensors that detect variations in blood volume in peripheral vessels produced by each cardiac contraction by projecting photons into body tissues and analyzing the reflected light. Such a PPG technique is one of the most widely adopted HR measuring technologies in smart devices produced these days [23].
Sampling frequency, defined by “the number of samples per second (or per other unit) taken from a continuous signal to make a discrete or digital signal,” is an important concept to better understand mechanism and pitfalls of PPG sensors. A higher sampling frequency indicates a higher accuracy of analysis because more data samples are collected in the same time interval [29]. Gold standard ECG used in this study collects data at the frequency of 512 Hz, and MC200 collects at the frequency of 256 Hz. The exact sampling frequency of AW7 and SW4 are not made public. While the sampling frequency of the previous Samsung Watch is estimated to be between 20–25 Hz [30,31], Apple describe that their HR monitor blink hundreds of times per second to measure HR, without mentioning the precise sampling frequency [32]. Likewise, the discrepancy in each sampling frequency may be an important reason for different accuracy between devices.
On the other hand, PPG sensors have some drawbacks. According to previous research, PPG sensors show low accuracy of HR measurements with darker skin likely because darker skin with more melanin absorbs more green light than lighter skin [29]. Moreover, the accuracy of PPG sensors are susceptible to motion artifact especially when the motion was cyclic or repetitive (e.g., walking and jogging). An accelerometer, which senses changes in velocity over time, is one of the methods used to detect motion artifact and filter this output as noise reference [29,33].
In this study, we established that the new devices demonstrate the high accuracy of HR measurements even in the high-intensity aerobic exercise and during a rapid change in HR. It could be attributable to advanced technologies such as algorithms for signal processing in the models released recently.
Still, there are several limitations in this study. First, there is an imbalance of the gender distribution of the participants with more male ones, probably due to male-dominant prevalence of CAD [34,35]. However, previous studies concluded that the effect of gender on HR accuracy is none or unlikely clinically relevant [35,36]. Second, participants with severe or sustained arrhythmia (such as atrial fibrillation or ventricular tachycardia) were not recruited for the study. The HR accuracy might decline when participants have such arrhythmias while measuring the HR. Third, participants held handrails in front of them for safety measures during the CPX. Since the hand position was fixed during the CPX, compared to regular running or jogging, the HR accuracy might have been overestimated with less motion artifact. Also, other aerobic exercises such as tennis, swimming, and skiing, or other forms of exercise such as resistance training may yield a different result.
Fourth, the results from this study may not be able to be generalized because only one device from each brand was used due to the cost. Some variations might be observed between devices when customers actually purchase these products. In addition, the effect of whether the wrist to wear a watch is left or right was not considered. One previous research concluded that neither left nor right hand wearing the device affected the accuracy of HR measurements [6]. Yet, it could have been more accurate if the hand wearing the device was randomized as part of an attempt to determine the factors affecting the accuracy of HR measurement. Also, even though one researcher helped the participants put on the devices as tight as possible, since the strap had holes in a straight line with regular interval for the users to fasten the strap, the devices could not be worn with fine adjustment. The tightness of the strap was decided without objective measurement of tension or pressure, but rather subjectively. Hence, the tightness of the devices might not have been consistent among participants. Lastly, although the HR values from all the devices were displayed on the monitor in real-time, we were not able to check all the values simultaneously. However, the time lag between HR records were less than a few seconds. As the electronics technology advances with newer products, additional studies that supplements such limitations will be necessary in the future.
In the present study, we evaluated the HR accuracy of wearable devices recently released during the CPX test performed by participants holding handrails. We concluded that new devices demonstrate the superior accuracy of HR measurement, compared to previous studies conducted with old devices even during the high intensity exercise. It is likely that cardiac patients participating in the high-intensity exercise under condition where HR is measured reliably, may benefit from utilizing these wearable devices. Also, as many people worldwide already own these watches, it will be helpful for both cardiac patients and healthy people when they do self-exercise.