INTRODUCTION
Poliomyelitis is a viral disease that is likely to develop in children. The paralysis caused by poliomyelitis tends to last for several days and wear off over several months. The survivors of initial poliomyelitis remain sufficiently stable maintain their lifestyles for decades. After 20 to 40 years' stability, however, 30% to 65% of polio survivors show late exacerbation [1,2,3,4,5,6,7] caused by the denervation that results from thickened nerves, chronically persistent viral infections, and internal and surgical complications caused by immune diseases, aging, post-polio syndrome, and other ailments [2]. In poliomyelitis, polioviruses disrupt motor nerves, and denervation occurs in the muscles that are controlled by nerves. Then, the new axonal sprouts of the surviving motor nerves reinnervate the denervated myofibers; in certain cases, however, the surviving motor nerves have abnormally bulky axons, and decades later, they have difficulty maintaining the axons as neuronal metabolism slows. As a result, polio survivors suffer from muscular weakness and atrophy and chronic pain and fatigue and are unable to exercise sufficiently, which leads to increased obesity as well as systemic and topical fat content.
The correlation between obesity and pulmonary function was first introduced in the late 1950s, and since then, many studies have been conducted to establish the influence of obesity on dynamic thoracic and pulmonary function. According to previous studies, obesity is known to cause chronic hypoxia caused by ventilatory defects, hypercapnia caused by respiratory failure, and respiratory diseases such as asthma and sleep apnea [8].
Compared with healthy people, polio survivors have a higher risk of restrictive lung disease [9] and hypoventilation [10] because they are more prone to respiratory muscle weakness, scoliosis, and the consequent thoracic deformation.
In previous studies, pulmonary hypofunction was cited as a symptom of post-polio syndrome, but there has been no study on the correlation between obesity and pulmonary function in polio survivors. Chang et al. [11] reported that polio survivors showed a higher incidence of obesity and a marked increase in fat mass; total body fat was at least 50% higher in polio survivors than in healthy people, and that fat was distributed systemically, especially around the thorax. These authors' results suggest that pulmonary hypofunction is closely linked to obesity in polio survivors.
The World Health Organization has reported that the number of polio survivors around the world has reached approximately 20 million. It is thus worthwhile to accurately analyze the relationship between obesity and pulmonary function.
This study thus focuses on identifying the correlation between obesity and pulmonary function in polio survivors.
MATERIALS AND METHODS
Subjects
This study was conducted on patients with poliomyelitis or post-polio syndrome who were recruited from Ewha Womans University Hospital, Seoul National University Bundang Hospital, Seoul National University Hospital, the SMG-SNU Boramae Medical Center, the National Rehabilitation Center, and the Hwaseong City Health Center. The inclusion criteria were being 40 years or older and diagnosed with poliomyelitis and having been treated within a sufficient period for the occurrence of polio sequelae. The study participants voluntarily signed consent forms acknowledging that they were willing to allow their personal and health information to be used or published and that they were willing to follow the study protocol and requirements. Patients who were illiterate, had difficulties in communicating or completing the questionnaire, or were uncooperative were excluded from the study.
All of the study procedures were approved by the local Institutional Review Boards, and all of the participants provided written consent.
Medical inquiry
The study survey consisted of questions regarding patients' genders, current ages, present paretic regions, ages and paretic regions at the time of diagnosis, physical activity levels, and comorbidities including diabetes, hypertension, cerebrovascular diseases, chronic obstructive pulmonary disease (COPD), tuberculosis (Tb), and asthma. Physical activity was classified into 11 categories in total: running, run-up, run-down, long-distance ambulation without orthosis, short-distance ambulation without orthosis, long-distance ambulation with orthosis, short-distance ambulation with orthosis, long-distance ambulation with crutches, short-distance ambulation with crutches, wheelchair ambulation, and other activities. Each item was scored on a scale of 0 to 1; a completed activity received a score of 1, and an unperformed activity received a score of 0.
Physical examination and obesity analysis
During the physical examinations, patients' weights, heights, body mass indexes (BMIs), and waist circumferences were measured. Body fat amount, body fat percentage (BFP), total body mass, and lean body mass were evaluated using the InBody 720 Instrument (Biospace, Seoul, Korea).
Muscular strength was evaluated based on the Medical Research Council (MRC) scoring system. The system scores muscular strength on a scale of 0 to 5 where 0 means that no movement is observed and 5 reflects normal muscular contraction against full resistance. In this study, the muscular strength test was conducted on both upper limbs and lower limbs, and the two values were averaged.
Pulmonary function test
The pulmonary function test was conducted on forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), and ratio of FEV1 to FVC, (FEV1/FVC) using a Vmax29 (SensorMedics, Yorba Linda, CA, USA) spirometer. The study participants breathed in and out as long as they could, following the doctor's instructions. When breathing out, they attempted to continue until they had no breath to exhale, and they attempted to not breathe in. Exhalation was measured until there was no airflow detected, the lung volume measured by the spirometer had plateaued, and air was exhaled for 6 seconds or longer.
FVC and FEV1 were converted into predictive values in percentages, according to a formula based on gender, age, height, and weight and revised based on Koreans' pulmonary functions [12].
In addition, the difference was calculated between chest circumference measured at the time of inspiration and at the time of expiration.
Statistical analysis
All data were statistically analyzed using SPSS ver. 14 (SPSS Inc., Chicago, IL, USA).
The Pearson chi-square test was used to examine the correlation between obesity and pulmonary function.
The partial correlation coefficient between obesity and pulmonary function was calculated using MRC scores and controlling for activity levels. The controlled MRC scores were for both hip flexors, hip extensors, knee extensors, shoulder flexors, shoulder abductors, elbow flexors, and elbow extensors, which was to control the muscles that are known to have enhanced pulmonary function when their strength was improved in previous studies [13,14,15,16,17].
Statistical significance was defined as p-value less than 0.05.
RESULTS
Demographic data
A total of 73 polio survivors participated in this study (Table 1). Of the 73 participants, 24 were males, and the other 49 were females. Their mean age was 51.33±7.78 years. At the time when they were diagnosed with poliomyelitis, their mean age was 2.25±1.33 years. At the time of diagnosis and more recently, a unilateral leg accounted for the highest percentage of paretic regions, 63.0% (46 patients). Physical activity levels averaged 5.61±3.71.
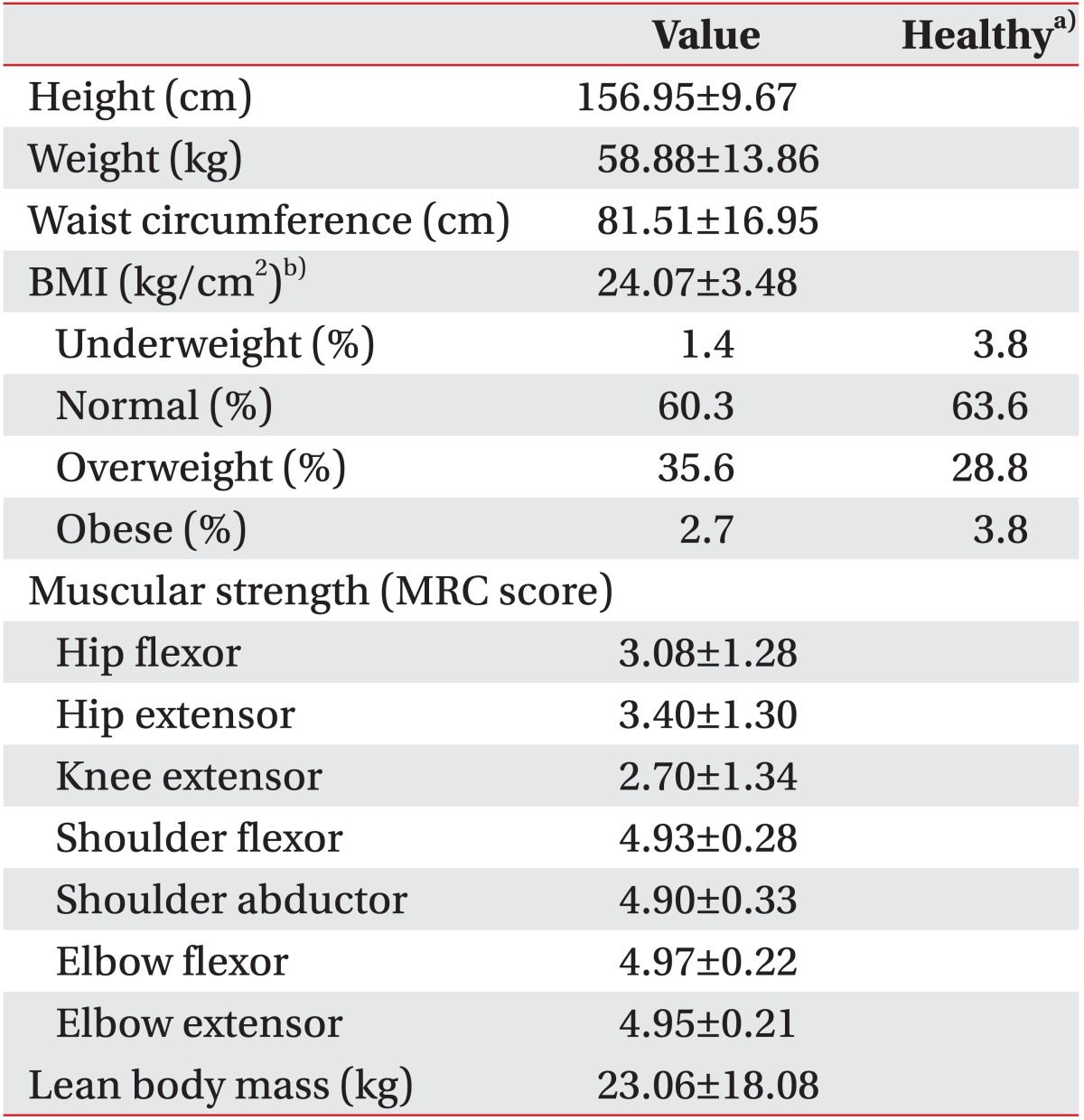
Hypertension accounted for the highest percentage, 24.7% (18 patients), of comorbidities. However, no patients had COPD, Tb, or asthma. Table 2 shows the mean values of BMI, lean body mass, and MRC muscle strength scores. Mean lean body mass was 23,057.56±18,079.30 g.
Obesity
The patients' BMIs were calculated based on their heights and weights. The degree of obesity was classified as follows: a BMI of less than 18.5 kg/m2 was defined as underweight; 18.5 to 24.9 kg/m2 was normal; 25 to 29.9 kg/m2 was overweight; 30 to 39.9 kg/m2 was obese; and 40 kg/m2 or higher was morbid/severely obese; mean BMI was 24.07±3.48 kg/m2 [18]. Forty-four patients (60.3%) were classified as normal, and 26 (35.6%) were overweight. Of the original 73 patients, 28 (38.3%) recorded a BMI of 25 kg/m2 or higher; their average waist circumference was 81.51±16.95 cm (Table 2).
Pulmonary function
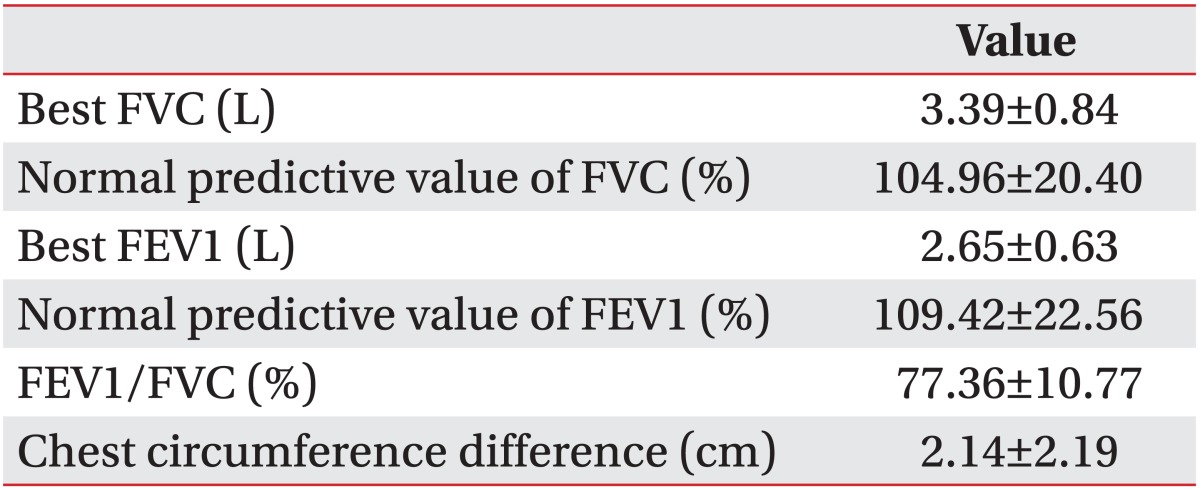
The best FVC measured by the pulmonary function test reached 3.39±0.84 L on average. The best FEV1 was measured at 2.65±0.63 L. The ratio of FEV1 to FVC was calculated to be 77.36%±10.77%. The circumferences, measured during inhalation and expiration, showed a difference of 2.14±2.19 cm (Table 3).
Correlation between obesity and pulmonary function
Pearson correlation coefficient was calculated for BMI and normal predictive value of FVC in polio survivors, which was measured at -0.30. The p-value was less than 0.05 and thus, the result was found to be statistically significant (Table 4). There was no significant correlation between the pulmonary function indexes excluding the predictive value of FVC and the obesity indexes excluding BMI.
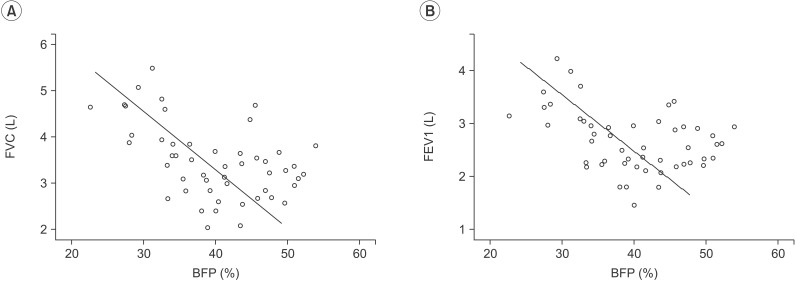
BFP had a negative correlation with the best FVC and the best FEV1, -0.60 and -0.50, respectively, in relation to MRC scores for hip flexors, hip extensors, knee extensors, shoulder flexors, shoulder abductors, elbow flexors, and elbow extensors with activity levels controlled for. The values were statistically significant (Table 5, Fig. 1).
By gender, Pearson correlation coefficient showed that BMI had a negative correlation with the best FVC, the normal predictive value of FVC, the best FEV1, the normal predictive value of FEV1, FEV1/FVC, and chest circumference in both males and females, although there was only statistical significance among the males.
DISCUSSION
The researchers of this study measured the subjects' BMIs, waist circumferences, BFPs, and total body fat amounts and found that BMI and BFP correlated with pulmonary function. Specifically, this study found that FVC was nearly inversely proportional to BMI and BFP among polio survivors. However, there was no significant correlation between BMI and FEV1/FVC or between BFP and FEV1/FVC. BMI is a convenient measure of obesity based on a ratio of weight to height [19], specifically, body weight divided by the square of height. However, bodies comprise many components such as fat, muscles, connective tissue, etc. Even people with similar BMIs differ in muscle mass, strength, and pulmonary function, which is why this study controlled for MRC scores and physical activity levels before examining the correlation between BFP and pulmonary function. The result was that BFP had a negative correlation with best FVC and best FEV1. However, there was no significant correlation between BFP and FEV1/FVC, as there was with BMI. This finding suggests that body fat negatively affects pulmonary function when muscular strength and activity levels are controlled for and thus may lead to restrictive lung disease.
This result is consistent with the study by Pistelli et al. [20], who reported that BMI was an important predictor related to FVC, as well as that by Fabris De Souza et al. [21], who reported that the lower the FVC, the more obese the patient. Similarly, Sin et al. [22] reported that BMI did not correlate with FEV1/FVC.
Restrictive lung disease is known to affect lower FVC, and obstructive lung disease is known to affect FEV1/FVC [23]. In this study, Pearson correlation coefficient was calculated regarding pulmonary function and obesity. It was found that FVC and BMI had a negative correlation, which is consistent with the previous study that found that the incidence of restrictive lung diseases was nearly proportional to BMI [24] as well as with previous studies that polio survivors were susceptible to restrictive lung diseases [25].
Many studies have been conducted on the influence of obesity on cardiopulmonary dynamic and pulmonary function [21,22], and the mechanism between obesity and pulmonary function may be explained by fat that has accumulated in the thoracic and abdominal cavities. The accumulation of fat is presumed to reduce lungs' elasticity, decreasing mechanical efficiency and increasing the daily oxygen demand [26,27]. As BFP increases, fat accumulates much more in the abdominal cavity, reducing thoracic volume and thereby reducing even vital capacity, which leads to respiratory muscle weakness and decreased mechanical efficiency. Moreover, increased BFP leads to decreased lung volume, makes respiration shallow and rapid, expands the respiratory dead space, causes airway obstruction and atelectasis, and ends with pulmonary dysfunction [26].
In addition, Pearson correlation coefficient showed that BMI had a statistically significant negative correlation with pulmonary function only among males, which can be explained as follows. Even when men and women have the same BMIs, males have android-type obesity and consequently accumulate fat around their abdomens and thoraxes. Women, however, have gynoid-type obesity, and fat tends to accumulate around their buttocks and lower limbs [28,29]. In this study, android fat and waist circumference were measured, and the partial correlation coefficient was calculated using BMI as a control variable. The result was that the men had more android fat and larger waist circumferences than did the women even when the pairs had the same BMIs. In other words, the men whose thorax and abdominal cavities contained more fat showed a statistically significant correlation between obesity and pulmonary function, which could support the hypothesis of this study that obesity causes fat to accumulate in the thorax and abdominal cavities and therefore causes pulmonary insufficiency.
This study showed a significant correlation between BMI and the normal predictive value of FVC. Given that other studies have found that height is correlated to pulmonary function [30], it was essential that we demonstrate that although height is a known factor of BMI, it did not affect our experimental results. With height as a control variable, a statistical analysis showed a strong negative correlation between the normal predictive value of FVC and BMI. Therefore, we could exclude height as a confounding variable.
In addition, this study's researchers examined the correlation between pulmonary function and the lean body masses of both upper and lower limbs using BMI as a control variable. The result was that the lean body masses of both upper and lower limbs had significant positive correlations with the best FVC, and the lean body masses of both upper limbs and the left lower limb had significant positive correlations with the best FEV1. These findings suggest that increased lean body mass in both the upper and lower limbs will enhance pulmonary function.
In this study, approximately 38% of the polio survivors recorded BMIs of 25 kg/m2 and higher, which was slightly more than the average among healthy Korean adults in general, 32.6% [31]. Polio survivors who do not get sufficient exercise are more likely to be obese and to suffer pulmonary dysfunction compared with healthy people. Previous studies found that polio survivors might suffer from pulmonary hypofunction because of muscular atrophy, muscular weakness, and thoracic deformation caused during the advanced deterioration [32]. In brief, polio survivors are more likely to become obese as pulmonary hypofunction arises from muscular weakness and thoracic deformation. This is why the risk of pulmonary function deterioration is much greater in polio survivors than in healthy people.
Pulmonary hypofunction is the most common complication in polio survivors; in fact, 27% to 58% of polio survivors suffer from respiratory problems such as shortness of breath, difficulty expectorating, and snoring [32]. Malfunctioning lungs can cause an imbalance between ventilation and perfusion, pneumonia, and pulmonary fibrosis, and in serious cases, patients are placed on ventilators [33]. Accordingly, there is the need to focus on preventing pulmonary hypofunction or slowing its progress.
In previous studies, pulmonary function was improved in patients whose BMIs decreased or who were otherwise no longer morbidly obese [34,35]. These results suggest that pulmonary function may be improved by weight reduction even in polio survivors with pulmonary hypofunction. However, it may be difficult for polio survivors with muscular weakness, contracture, and other sequelae to exercise according to weight reduction programs that are designed for healthy people. Leith and Bradley [36] asserted that respiratory muscle training could improve respiratory muscle strength and endurance. As stated in the introduction, poliomyelitis-related hypoventilation leads to hypercapnia, dyspnea, fatigue, and even hypoactivity, any of which could cause obesity; in this regard, respiratory muscle training is expected to play an important role in breaking the cycle of increasing weight and decreasing lung function. It is necessary to develop exercise programs specifically for polio survivors who need to reduce their weight and strengthen their respiratory muscles, and additional research would be necessary as well.
However, this study does have a number of limitations. First, in this study, visceral fat, maximal inspiratory pressure (MIP), and maximal expiratory pressure (MEP) were not measured. Computed tomography (CT) can measure visceral fat amount and distribution, and MIP and MEP can measure how much inspiratory and expiratory muscles have been weakened. If visceral fat, MIP, and MEP had been measured, it would have been more helpful in explaining how obesity negatively affected pulmonary function in polio survivors. A second limitation is the gender imbalance; the ratio of males to females was 1 to 2.04. A third was the small number of subjects, 73 in total, and the absence of any control group composed of healthy people. Thus, an additional study needs to be conducted to compare polio survivors with healthy people and males with females.