INTRODUCTION
Acute poliomyelitis, which occurred worldwide in the early and mid-twentieth century, has now been nearly eliminated and has become a rare condition. New cases are seldom reported because of the advent of effective vaccination; but, it still exists in some developing countries [1,2,3]. However, a large number of polio survivors are still alive today and are suffering from residual disability. The estimated number of people affected by poliomyelitis is around 15 million worldwide [4].
Especially, clinicians have focused on the late effects of poliomyelitis, such as post-polio syndrome (PPS), secondary musculoskeletal problems, obesity, etc. Polio survivors experienced a variety of new neurological, musculoskeletal, and systemic symptoms, such as cold intolerance following a stable period after acute infection [5]. The constellation of these symptoms is referred to as PPS. Although numerous studies with respect to the etiology of PPS have been performed, the pathogenesis of PPS has not been completely understood [6,7]. Some studies suggested that the pathophysiology of PPS is attributed to distal degeneration of axons of the greatly enlarged motor units that developed during recovery following acute paralytic poliomyelitis [4,8]. The symptoms of PPS could be severe enough to impair the overall quality of life, significantly deteriorate work-related function, and impose lifestyle changes [5]. Additionally, polio survivors might be at high risk of having multiple medical comorbidities and falling [9,10,11,12]. Although the prevalence of PPS was reported to be in a varying range, it is definitely a common neurological disorder that occurs in a large proportion of polio survivors [13,14,15]. Therefore, in Europe and North America, many prospective cohort studies are being performed to analyze the relationship between the late effects of polio or PPS and the quality of life in polio survivors [10,16,17,18].
However, in Asian countries including Korea, few studies about polio survivors have been reported and a prospective cohort study has not yet been performed. Therefore, the socioeconomic, medical, and functional problems of polio survivors who became middle-aged or old adults are not well known in these regions. Therefore, it is necessary to investigate the overall data of polio survivors in a nationwide study, and this information would be helpful in understanding their potential or neglected problems.
The present study was designed to obtain information on the socioeconomic, medical, and functional status of polio survivors by telephone interview, and to use the results of this survey as the preliminary data for establishing the middle-aged cohort of polio survivors.
MATERIALS AND METHODS
Subjects
All candidates were patients who were previously diagnosed with poliomyelitis or poliomyelitis with post-polio sequelae according to their medical records. Contact information including the name, address, and telephone number was obtained from the medical records of Seoul National University Bundang Hospital, Seoul National University Hospital, SMG-SNU Boramae Medical Center, National Rehabilitation Center, Chonnam National University Hospital, Gyeongsang National University Hospital, Ewha Woman's University Hospital, Hwaseong City Health Center, and Jeongnip Welfare Center. After the interviewer introduced himself or herself, past medical history of poliomyelitis infection was confirmed again when the subjects were contacted initially by phone. Before conducting the survey, the purposes of this study, which were to investigate the general data of polio survivors and to establish the middle-aged cohort of these patients, were explained to the subjects. Upon agreement of the subjects to participate in the study, a structured questionnaire was administered over the phone. The study and all procedures were approved by the Institutional Review Board of Seoul National University Bundang Hospital.
Methods
The questionnaire contained detailed questions about the following: the age of onset of poliomyelitis, the presence of upper and/or lower limb paralysis, the presence of newly developed symptoms which reduced his/her physical function, such as fatigue, weakness, and/or pain related to PPS and the onset of these symptoms. Interval between acute poliomyelitis and the onset of symptoms related to PPS was determined as a result. Use of orthoses or walking aids, current ambulatory function, the disability rating registered in national welfare system, self-reported health status, past medical history including surgical treatments, history of falling in the last one year and medical comorbidities were evaluated. For the detailed analysis, history of surgery was investigated. Orthopedic surgeries, such as correction of length discrepancy of lower limbs or deformation of joints, were categorized as surgeries related to sequelae of poliomyelitis. However, simple fracture surgeries after falling down were excluded. With respect to the socioeconomic domain, the questionnaire included various questions about marriage, cohabitant, residence, religion, academic background, monthly family income, and occupation. The survey consisted of 39 questions with respect to the medical, functional, and socioeconomic domains (Table 1). Although the patients agreed to participate in this study, the subjects were allowed to skip some of the questions and the answers to these questions were categorized as missing values.
The telephone interviews were performed by trained interviewers including two physicians and three research nurses. Prior to the beginning of the interview, several meetings were held to revise the questionnaires and to educate the interviewers about poliomyelitis, sequelae of poliomyelitis, post-poliomyelitis syndrome, etc. The questionnaire was modified once during this process.
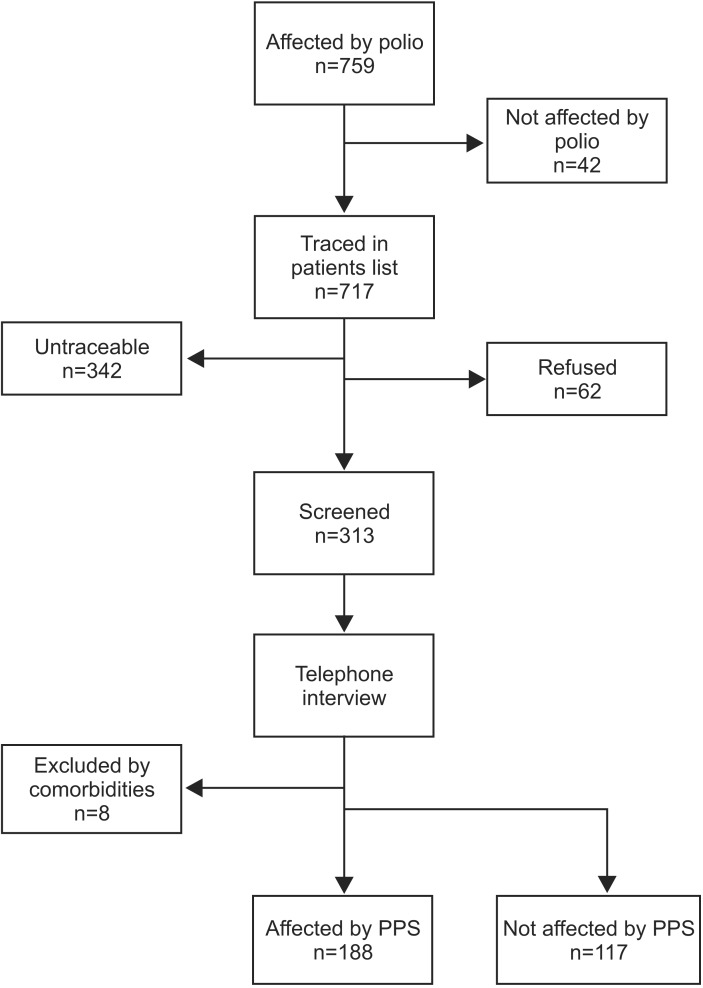
The diagnostic criteria for PPS were adopted from the European Federation of Neurological Societies (EFNS), whose guidelines are commonly used to diagnose PPS [19] (Table 2). Subjects who met all the criteria were categorized into the PPS group. Subjects who had cerebrovascular diseases were excluded from the PPS group because their newly developed symptoms might not be related with PPS (Fig. 1).
Statistical analysis
All statistical analyses were performed with PASW statistics ver. 18 (http://www.winwrap.com). Descriptive statistics for the demographic and socioeconomic data were computed. Differences in the frequencies between groups were tested by χ2 analysis. We used the median of the distribution in all of the subjects to determine the cut-off for dichotomising continuous variables. Univariate analysis was performed to identify the possible risk factors of PPS. The association between a risk factor and PPS was expressed using odds ratio (OR) with 95% confidence interval (CI). Risk estimates were adjusted for the effect of all other factors using multiple logistic regression models. Statistical significance was accepted at p<0.05. All p-values were two-sided.
RESULTS
The characteristics of subjects
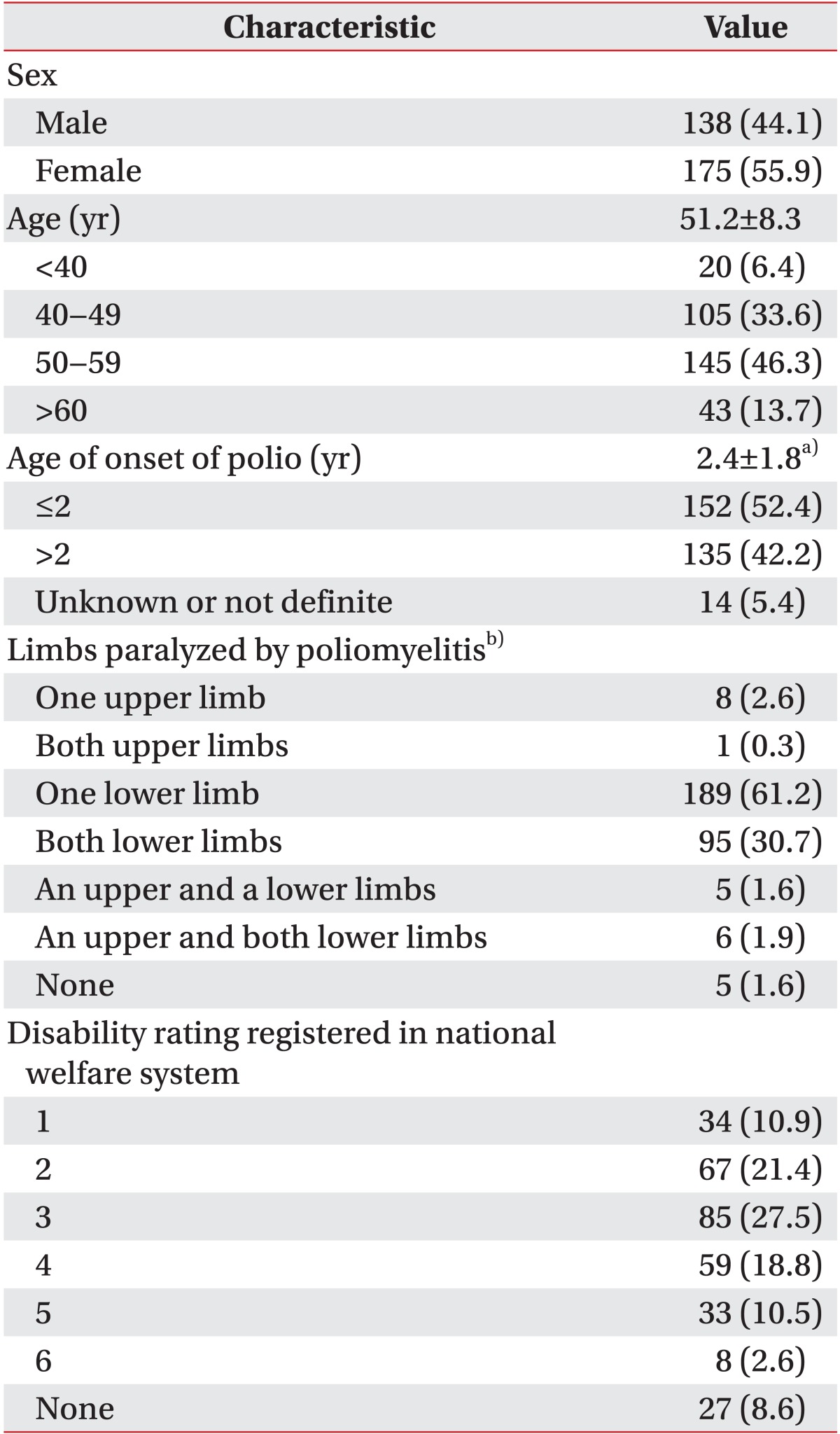
Fig. 1 shows the flow chart of the steps for identifying patients affected by PPS. A total of 759 subjects were registered in our database from 9 centers consisting of 6 university hospitals, a national rehabilitation center, a city health center, and a welfare center. This number represents approximately 1.9% of estimated polio survivors extracted from the database of 'National Survey of Disabled Persons 2011', which is a survey conducted by the Korean government every 3 years. Among them, 42 subjects did not have a history of acute poliomyelitis based on the initial review of specific medical records. Among the remaining subjects, 342 subjects could not be contacted due to incorrect contact phone number or change in the contact phone number, and 62 patients declined to participate in the interview. As a result, a total of 313 polio survivors completed the questionnaire via a telephone interview (response rate 83.5%). The demographic and etiologic characteristics of participants are summarized in Table 3. The mean age of polio survivors was 51.2±8.3 years (median 52 years; range 19-80 years) and 60.0% of patients were above 50 years of age. Also, 55.9% of patients were females. The mean age at onset of acute poliomyelitis in all of the subjects was 2.4±1.8 years (median 2 years; range 0-12 years). More than half of the patients (52.4%) suffered from the acute infection at or below 2 years of age.
Medical, functional, and social problems
The large majority of the subjects had paralytic poliomyelitis involving the lower limb(s) (Table 3). Three-fifths of the subjects had paralysis in only one of the lower limbs (61.2%), and 30.7% of the subjects had symptoms in both the lower limbs. The occurrence of paralysis in the upper limbs was relatively rare. More than 90% of the subjects had disability ratings registered in national welfare system (91.4%). About three-fifths of the subjects had a severe level of disability of grade 3. About half of the subjects could walk more than 500 m with or without an orthosis or a walking aid (54.0%). Also, 49.8% of the subjects could go up and down the stairs. Only one-fifth of the patients could run (18.7%). Also, 69.0% of the polio survivors had fallen within the last one year and about two-fifths of them reported at least one fall per month. In addition, 32.0% of the polio survivors who experienced a fall in the past one year had sustained an injury as a result of the fall. The common sites of injury were lower limbs (74.2%), upper limbs (29.2%), lower back (5.6%), chest (3.4%), abdomen and pelvis (3.4%), and head (1.1%). The injuries included bruising (33.3%), laceration and abrasion (31.8%), bony fracture (30.3%), and tendon injury (13.6%).
According to the self-reported health status, about onefourth of the polio survivors perceived that their health status was relatively poor (poor or very poor; 26.5%) and only 35.2% of the polio survivors felt that they were healthy (very good or good). Common chronic comorbidities, such as hypertension (26.8%), diabetes mellitus (13.8%), gastric ulcer (9.4%), liver disease (3.1%), kidney disease (3.1%), and cerebrovascular disease (2.6%) were reported. About three-fifths of the subjects used health care services for poliomyelitis sequelae (59.7%) and orthopedic surgeries were the most common among them (73.3%). More than one-third of the subjects (n=126) did not get any medical services for sequelae of poliomyelitis and 37.3% of them wanted to get health care services for their problems.
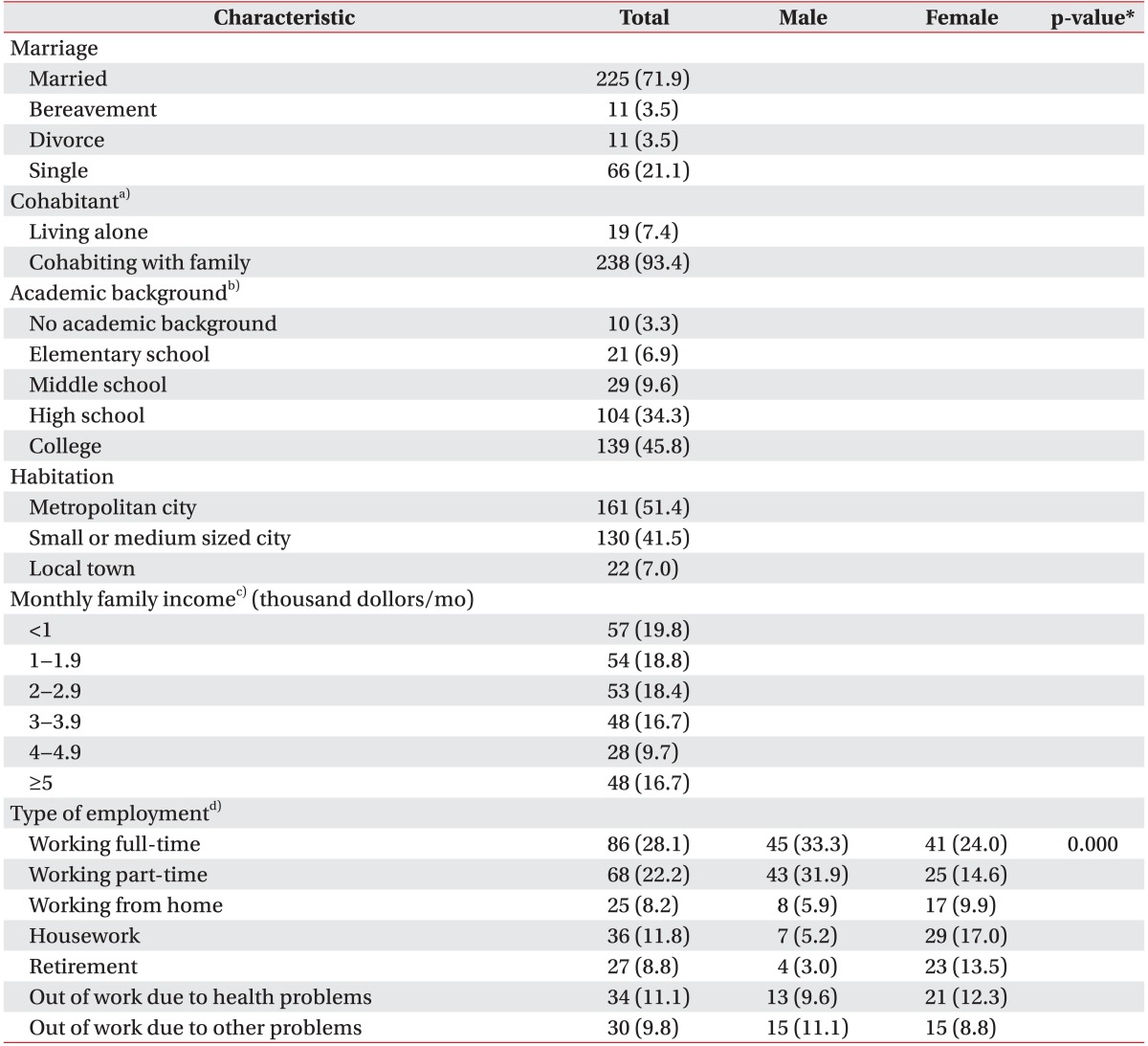
Socioeconomic characteristics of the subjects are summarized in Table 4. The large majority of participants were married (71.9%) and a few were bereaved or divorced respectively (3.5% and 3.5%). Only about one-fifth of subjects were single (21.1%) and less than one-tenth of subjects were living alone (7.4%). Most of the subjects received high school education or higher education than high school (77.6%). About half of the subjects lived in a metropolitan city (51.4%) and the rest lived in a small or medium sized city or a local town. Monthly family incomes were found to vary among the subjects. About one-fifth of their families made less than one thousand dollors per month (19.8%), and 29.7% of the polio survivors did not have a job, 8.8% of the polio survivors retired at the regular retirement age, and 11.1% of the polio survivors were out of work because of their health problems. The type of employment differed significantly according to the gender (p=0.00) (Table 4).
Late effects and risk factors for post-poliomyelitis syndrome
A total of 61.6% of the subjects (n=188) met the adopted diagnostic criteria for PPS (Table 5). The mean age of patients in the PPS group was 51.3±7.9 years and that of patients in the non-PPS group was 50.6±8.9 years. The mean age of patients in both groups did not show a significant difference (p=0.408). The time interval between acute poliomyelitis and development of PPS was 38.5±11.6 years. Fatigue or decreased endurance was the most commonly reported newly developed symptom following a period of years of stability after acute poliomyelitis in the PPS group (80.9%). Also, 65.6% of the patients in the PPS group reported weakness in their limb(s). They experienced weakness in their limb unaffected by acute poliomyelitis (41.5%), and 55.9% of patients in the PPS group experienced pain in their limb(s). The tendency for distribution of joint pain was similar to that for weakness. Pain also developed in both limb(s), regardless of paralysis. Also, 58.5% of patients in the PPS group reported wasting of limb muscles. Lower back pain was the most common symptom (18.4%) except above major three symptoms, and the other symptoms included deformity of limbs, scoliosis, edema, joint stiffness, etc.
There was no statistically significant difference in the distribution and the number of paralyzed limbs between the PPS and non-PPS groups. Significant differences were not found in the items related to ambulatory function and fall history within the recent one year between the PPS and non-PPS groups. The presence of PPS did not affect the results of self-perceived health status. Among the subjects who did not get proper healthcare services, healthcare needs of patients in the PPS group were greater than those of patients in the non-PPS group (p=0.015).
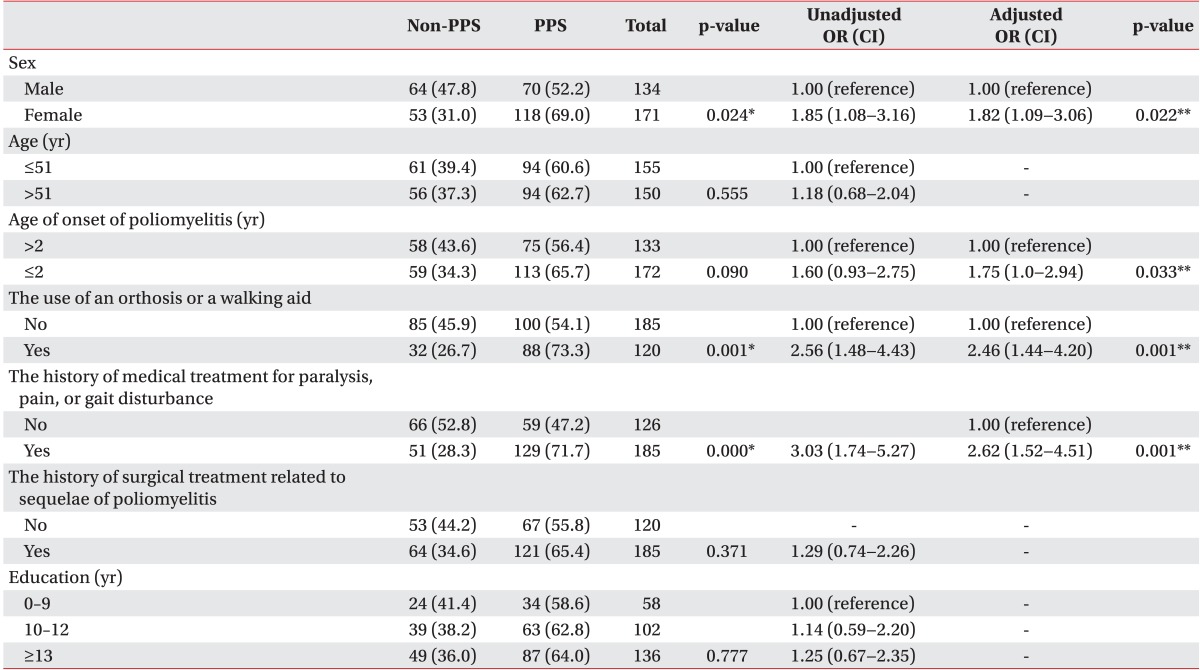
Univariate analysis of risk factors for PPS showed a significant association with female gender, the use of orthoses or walking aids, and history of medical treatment for paralysis, pain, or gait disturbance (Table 6). In multiple logistic regression analysis , these factors were confirmed and early age of onset of poliomyelitis was added as an independent risk factor for the development of PPS. Various variables, such as the academic background, the economic ability, the type of employment, and so on, were applied to univariate analyses as the risk factors for PPS. However, these variables did not have any statistical significance.
DISCUSSION
In this survey, we found that the mean age of polio survivors was more than 50 years and they had begun to enter middle age, and the prevalence of PPS was 61.6%. Most of the polio survivors had paralysis of the lower limb(s) as the sequelae of poliomyelitis and showed ambulatory dysfunction. They were exposed to high risk of fall, and about one-fourth of them reported that their health status was relatively poor. One out of ten patients had to quit his or her job due to the health problem. The need for healthcare services in patients of the PPS group was greater than that in patients of the non-PPS group. Female gender, early age of onset of poliomyelitis, the use of orthoses or walking aids, and history of medical treatment for paralysis, pain, or gait disturbance were found to be the significant risk factors for the development of PPS.
The prevalence of PPS was reported to range from 15% to 80% because of differences in the criteria applied and the population studied [13,20,21,22,23,24]. These results demonstrated that 78.0% of the total subjects developed at least one symptom, such as fatigue, pain, or weakness after a long period of stabilization following acute poliovirus infection and 61.6% of the subjects met the clinical diagnostic criteria for PPS. In spite of the narrower criteria for PPS, the prevalence of PPS was reported to be much higher than 47.1% in a previous study of PPS in Korean polio survivors published in 2000 [25], in which the mean age of patients in the PPS and non-PPS groups was 40.1 years and 35.1 years, respectively. The mean age of polio survivors of 51.2 years, which was demonstrated in the current survey, indicates that the population continues to grow old with the passage of years. In addition, the time interval between the episode of acute paralytic poliomyelitis and PPS was reported to be about 38.5±11.6 years on average. This time interval was much longer than that of 27.6±10.0 years in the previous study of Korean polio survivors [25]. Taken together, the prevalence and duration of PPS are expected to increase with aging of this population.
Higher prevalence and increasing time interval between acute poliomyelitis and PPS indicate that the development of PPS could be linked with the aging process in polio survivors. This can be explained well by the pathophysiology of PPS, although it remains unclear. Motor units, which become pathologically larger after the recovery from acute poliomyelitis, undergo a continuous remodeling process through denervation and partial reinnervation, and it ultimately results in degeneration and defective neuromuscular transmission with aging due to failure of residual motor neurons to support and maintain collateral sprouting [4]. Therefore, we need to have a comprehensive plan for middle-aged polio survivors to detect newly developed symptoms and functional deterioration caused by PPS. Regular screening tests and function evaluations should be considered, especially in polio survivors with multiple risk factors for PPS.
We identified the following risk factors for PPS: female gender, early age of onset of poliomyelitis, the use of orthoses or walking aids, history of medical treatment for paralysis, pain, or gait disturbance. Several previous studies have also reported female gender, age at onset of poliomyelitis as the risk factors for PPS [13,20,26,27,28,29]. Several studies reported that disease severity was associated with risk of PPS [16,20,28]. However, the severity of acute poliomyelitis could not be determined clearly since the detailed neurological records were not available for most of the patients, and even if they were available, there was no grading or evaluating scale to indicate the severity of poliomyelitis. Hence, one of the studies assumed that the use of orthoses and aids during the recovery could reflect the magnitude of impairment caused by acute poliomyelitis, and another study used a numeric indicator for determining muscle involvement in poliomyelitis [26,29]. Although we could not check the number of muscles affected by poliomyelitis due to the limitation of telephone interview, we could evaluate the disease severity based on the dependency on orthoses or walking aids and history of medical treatment including surgery due to sequelae of poliomyelitis. We tried to investigate the socioeconomic factors as risk factors for PPS. However, we could not identify any significant associations.
Lower limb remained paralyzed after recovery from the acute episode of poliomyelitis in more than 90% of the total subjects. This could be mainly responsible for prominent ambulatory dysfunction. Only 18.7% of the subjects could run and 49.8% of the subjects could go up and down the stairs. They reported to have a problem with gait endurance. Moreover, about two-fifths of the patients needed orthoses or walking aids for ambulation. However, the temporal relationship between dependency on orthoses or walking aids and PPS was somewhat ambiguous. It may not be a risk factor for PPS because the current ambulatory dysfunction could be aggravated by PPS, and consequently patients in the PPS group might have become more dependent on orthoses or walking aids. To clarify this, it is necessary to determine when the subjects began to use the current orthoses or walking aids although this is not included in this survey.
Fall was a very common accident in polio survivors. They had fallen at least once in the past one year (69.0%). The frequency of fall was similar to that in other studies [11,12]. A large proportion of fallers experienced a bony fracture as a result of the fall (30.3%). We did not find a significant difference in the frequency of a fall accident between the PPS and non-PPS groups. Some studies have focused on osteoporosis in an aging post-polio population [30,31,32]. Osteoporosis occurred commonly in a postpoliomyelitis population. Considering the high risk of fall and progression of osteoporosis in aging polio survivors, prevention programs that aim to prevent falls are needed. Bone density assessment, review of fall risk, and therapeutic intervention should be considered in all of the polio survivors with a long-term management. Traditionally, muscle strengthening exercises for the lower limbs have been recommended for preventing fractures caused by falls because hip bone density was found to be strongly associated with muscle strength in the same limb [32]. However, the actual strengthening is limited to the atrophied or paralyzed limbs of polio survivors. Hence, we need to perform further researches on the therapeutic efficacy of exercise interventions specific for polio survivors.
There was no significant difference in the distribution of disability rating between the PPS and non-PPS groups. However, it would be meaningless to judge the current functional ability of polio survivors based on the disability rating because it was determined quite a long time ago, during the stable period after acute infection of poliomyelitis. Surely, long-standing poliomyelitis sequelae including PPS could affect their current functional ability [5,33]. Hence, regular functional evaluation is necessary in middle-aged or old polio survivors so as not only to screen for PPS, but also to re-evaluate the disability rating periodically because of the possibility of functional deterioration with aging.
The major limitation of this study was that all of the results were obtained via a telephone interview-based survey. The average time to complete a survey in one subject was about 30 minutes. This may affect the compliance and sincerity of participating in the survey. Secondly, proper assessment of PPS patients is not simple because of the non-specific nature of many symptoms and the influence of other features, such as psychological and physical factors. There were some studies on PPS using subtly different diagnostic criteria [26,29,34,35,36]. In our study, we adopted the criteria for the diagnosis of PPS recommended by EFNS task force, which are accepted as the universal criteria. Although we interviewed the patients carefully and thoroughly, we could not rule out other neurologic, medical, and orthopedic conditions which could be the cause of PPS symptoms due to lack of objective assessments. Only patients with cerebrovascular diseases which could affect the symptoms evidently were excluded from the PPS group. We assumed that other comorbidities, such as diabetes mellitus, liver and kidney diseases, are not related directly to muscle atrophy, joint pain and weakness. The possibility of overdiagnosis of PPS persisted.
In conclusion, we found that the majority of Korean polio survivors had begun to enter middle age with many medical, functional, and social problems. Female gender, early age of onset of poliomyelitis, the use of orthoses or walking aids, and the history of medical treatment for paralysis, pain, or gait disturbance were identified as the significant risk factors for PPS. The results of this study would be primarily used in a further study designed as a face-to-face visit and for establishing the middle-aged cohort of polio survivors. Consequently, a comprehensive and multidisciplinary plan needs to be prepared to manage polio survivors considering the highly prevalent multi-domain problems and risk factors for late effects, such as PPS.