INTRODUCTION
Balance, defined as the ability to maintain postural equilibrium, plays an important role in the performance of general movements in daily life [1]. In older adults, balance is crucial for postural stability when performing activities of daily living. Balance is achieved by the active control of body postures and movements in space with respect to gravity and the environment system based on sensory information from the visual, somatosensory, and vestibular systems [2]. For balance control, sensory inputs associated with the external environment, head orientation in relation to gravity, and body postures and movements according to the support surface are obtained from the visual, vestibular, and somatosensory systems, respectively [3]. For effective postural balance, the central nervous system must combine information from these three sensory receptors, and gradual impairment of their functions leads to impaired balance in older adults [4].
Impaired muscle strength and balance control are major risk factors for falls in older adults and have become an increasingly important issue. Falls affect one-third of community-dwelling older adults (≥65 years) at least once a year [5]. A variety of approaches for preventing falls and increasing muscle strength and balance control in older adults have been developed worldwide. Strategies include virtual-reality (VR) balance training using Nintendo Wii [6] and other devices and programs to improve muscle strength [7], balance control [8], and physical activity [9]. However, most of the devices developed and applied in fall-related intervention studies have limitations, such as an exclusive focus on muscle strength, balance, or cognitive performance and declining concentration and perseverance of older adults [10]. The American College of Sports Medicine reported that multidimensional physical activity programs for muscle strength, balance, and flexibility exercises efficiently improve physical health and body function in older adults [11]. In our study, an integrated multidimensional training device was used to simultaneously improve balance, muscle strength, and cognitive performance, and various exercises were combined with games to enhance the user’s concentration and perseverance. We hypothesized that muscle strength, balance, and cognitive performance of older adults could improve with strength and balance training using an integrated training device in combination with various rehabilitation exercises and games. Furthermore, we presumed that this device may be helpful to counter frailty in older adults, improve their physical performance and cognitive ability, as well as prevent sarcopenia. Accordingly, this study examined the role of the training device to simultaneously improve upper and lower extremity muscle strength, postural balance, and cognitive performance.
MATERIALS AND METHODS
Participants
This study was an investigator-led clinical trial and the number of participants was decided based on clinical findings at the discretion of the principal investigator (PI). Twenty older adults (11 males and 9 females; mean age, 70.70±2.81 years) who were capable of independent living were recruited, and each participant understood the purpose and procedure of this study and provided voluntary consent to participate in the clinical trial.
A two-sided test was used for sample size calculation, with the significance level α, power, mean change, and standard deviation set to 0.05, 80%, 0.47, and 0.697, respectively. The total number of participants was 20 [12].
The exclusion criteria were as follows: untreated serious internal or surgical diseases, severe cognitive impairment or aphasia that could impede following the investigator’s instructions, severe musculoskeletal abnormalities or damage in the lower extremities, or other conditions judged by the PI to be unsuitable for participation in the clinical trial. Individuals with no damage to the musculoskeletal system to the extent that exercises could not be performed due to paralysis or amputation, were permitted to participate in this study. Twenty participants, recruited from a senior welfare center using a poster advertisement, participated in the clinical trial, which was conducted from November 19, 2019 to March 13, 2020. This study was approved by the Institutional Review Board of Chonbuk National University Hospital (IRB No. CUH 2019-09-026). Each participant signed the IRB-approved informed consent form, and the participants’ rights were protected in accordance with the ethical principles of the Helsinki Declaration.
Training device
An integrated training device for strength and balance (SBT-120; Man&Tel Inc., Gumi, Korea), licensed as No. 19-944, was used in this study. This device was designed to simultaneously perform muscle strength, balance, and cognitive training and consists of a monitor, Kinect sensor, personal computer, wireless keyboard, safety frame, footpad, slings, and inertial measurement unit (IMU) sensor. The Kinect detects the user’s motion with a motion sensor camera, and the monitor displays the output of the user’s motion detected by the Kinect and the game-based training and measurement screens. The footpad is divided into nine sections, with a weight sensor installed on each section used to measure the weight of each section and to identify the user’s standing position. Two pairs of slings are placed above and below the device for the pull exercise using the muscle strength of the upper and lower extremities, respectively. The IMU sensor is configured to indicate its position on the monitor screen when the user moves his/her hand up and down while holding the sensor.
The game types used in this study included the hang glider game using the upper extremity slings, a submarine game using an IMU sensor, a stamp game using the lower extremity slings, and an arrow game using the footpad. In the hang-glider game, the hang glider moves to the left or right as the left or right hand moves the sling horizontally and up (flying) and down (landing) when both arms move the slings vertically (Fig. 1A). In the submarine game, participants can score points by catching fish in 6 minutes, including 3 minutes with the IMU sensor in the right hand, with the user adjusting the vertical position of the submarine raising the right arm to 90° and moving the sensor up and down while looking at the screen, and similarly for another 3 minutes with the IMU sensor in the left hand. In the stamping game, the participant can score points by identifying the correct direction and shape of the stamp as the one displayed by moving to the center and pulling the sling of the leg matching the direction. In the arrow game, the participant can score points by following the order of the arrow presented below the footpad using nine sections numbered from one to nine (Fig. 1B).
A 30-minute training session was conducted three times a week for 6 weeks; thus, a total of 18 training sessions were administered to all participants over the study period. The training frequency was set to three times a week in consideration of the participants’ scheduling constraints. A prior study compared the exercise effects of different training frequencies (one, two, and three times per week), and an exercise frequency of at least three times per week was recommended [13]. Participants performed each of the four training programs (two upper and two lower extremity exercises) for 6 minutes, followed by a 2-minute rest and preparation for the next training preparation.
Each game was divided into three difficulty levels: easy, moderate, and challenging. The easy-level training program tasks were presented for the first three sessions so that the participants could familiarize themselves with the device, and were then followed by the moderate-level tasks for the next five sessions (4–9), and by the challenging-level tasks for the remaining nine sessions (10–18). The difficulty level increased with decreasing time to recognize the presented game elements and the time to initiate an activity.
To prevent falls while using the device, safety measures were implemented by installing handles on both sides of the device.
Evaluations
The baseline performance of each of the 20 participants was measured using the Korean Mini-Mental State Exam (K-MMSE), Korean version of Montreal Cognitive Assessment (K-MoCA), Berg Balance Scale (BBS), Timed Up and Go Test (TUG), Functional Reach Test (FRT), manual muscle testing (MMT), and safety testing. The MMT was performed using the Nicholas manual muscle tester.
BBS is a balance ability measurement tool with a reliability of 0.97 and a consistency of 0.97 [14]. The BBS consists of 14 items, rated on a 4-point scale, with a maximum total score of 56 points. The TUG measures the time taken to stand up from a chair, walk 3 m, turn around 180°, walk back to the chair, and sit down [15]. The BBS and TUG have been widely used to assess the balance ability of older adults [16]. The reliability of the TUG test has been demonstrated to be 0.94.
FRT is a clinical measure of the ability to reach forward with an arm, as expressed by the distance (in cm) of the third metacarpophalangeal joint (middle finger knuckle) traveled from the starting position to the maximum forward reach of the arm outstretched while maintaining its horizontal level at 90° of shoulder flexion. A study tested the reliability of the FRT in 128 adults (20–80 years) and showed high reliability of 0.92 [17].
The K-MMSE was used for cognitive function evaluation, which is the most widely used dementia screening test in Korea; the K-MoCA showed a significant positive correlation with the K-MMSE and had high reliability (0.85) as a screening test for mild cognitive impairment [18].
Upon completion of training, a test-retest evaluation was performed, after a 4-week interval, to observe the persistence of the training effect. In the period between test and retest, participants were instructed to limit their activities to those of daily living. In the retest, changes in muscle strength, balance, and cognitive performance were determined. The rater held a master’s degree with a biomedical engineering major and had at least 3 years of clinical trial experience.
Statistical analysis
Descriptive statistics (mean and standard deviation) were used to analyze continuous variables, such as age, height, and weight, and frequency counts and percentages for categorical variables, such as sex.
Changes in evaluation items were observed at three time points: baseline (T0), immediately after training (T1), and four weeks after training (T2). Normality was evaluated using the Shapiro-Wilk test, followed by repeated-measures analysis of variance (RM-ANOVA) when normality was satisfied or the Friedman test as a nonparametric alternative when normality was not satisfied. For a significant difference detected by RM-ANOVA or Friedman test, a contrast test was performed for each time point using the Bonferroni or Wilcoxon signed-rank test, respectively, and the significance level was set at p<0.017.
RESULTS
Improvement in balance
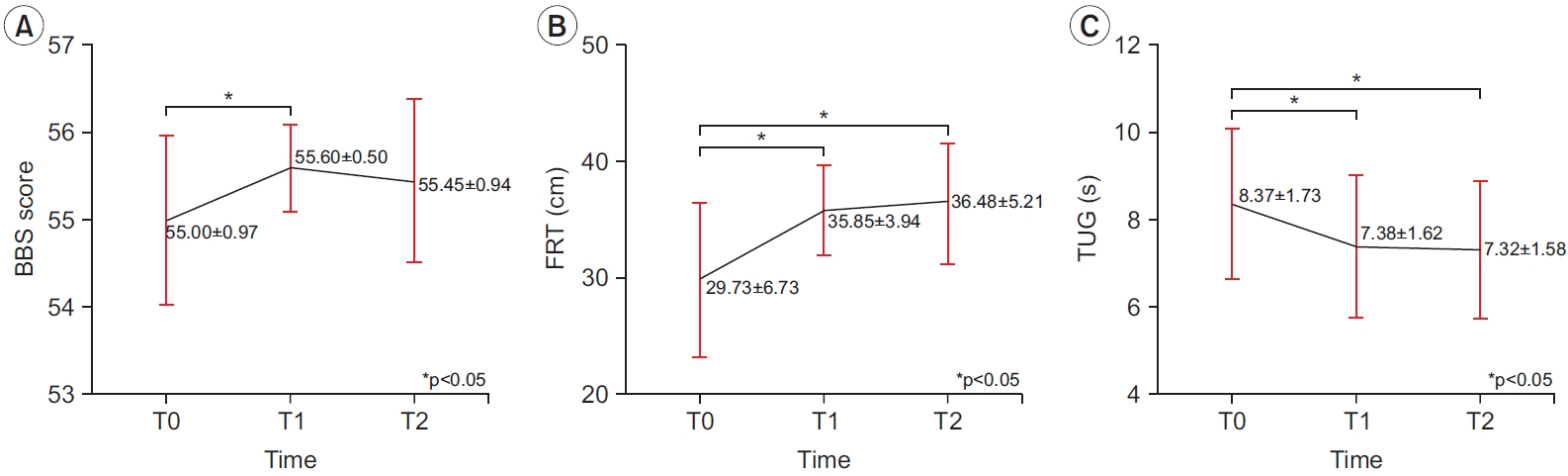
BBS scores at T0, T1, and T2 were 55.00±0.97, 55.60±0.50, and 55.45±0.94, respectively, which showed a trend toward a significant statistical difference but were not significantly different in clinical terms (p=0.033) (Table 1). Mean BBS scores increased by 0.6±0.94 from T0 to T1 (p=0.013) and 0.45±1.15 from T0 to T2 (p=0.103) but decreased by 0.15±0.93 from T1 to T2 (p=0.564; Fig. 2). FRT values at T0, T1, and T2 were 29.73±6.73, 35.85±3.94, and 36.48±5.21 cm, respectively, which were significantly different (p<0.001) (Table 1). Mean FRT values increased by 6.13±4.26 from T0 to T1 (p<0.001) and 6.75±4.79 from T0 to T2 (p<0.001) but decreased by 0.63±3.92 from T1 to T2 (p=0.501) (Fig. 2). TUG values at T0, T1, and T2 were 8.37±1.73, 7.38±1.62, and 7.32±1.58 seconds, respectively, which were significantly different (p=0.015) (Table 1). Mean TUG values decreased by 0.99±2.00 from T0 to T1 (p=0.037), 1.05±1.55 from T0 to T2 (p=0.007), and 0.06±0.76 from T1 to T2 (p=0.411) (Fig. 2).
Improvement in muscle strength
MMT values measured with the Nicholas MMT showed improvements in all joints. The largest improvement in muscle strength was found in the right shoulder joint in the upper extremities, as well as the right hip joint in the lower extremities. Their left-side counterparts also showed the greatest improvement, but the improvement extent was not as much as that on the right side (Tables 2, 3).
Improvement in cognitive performance
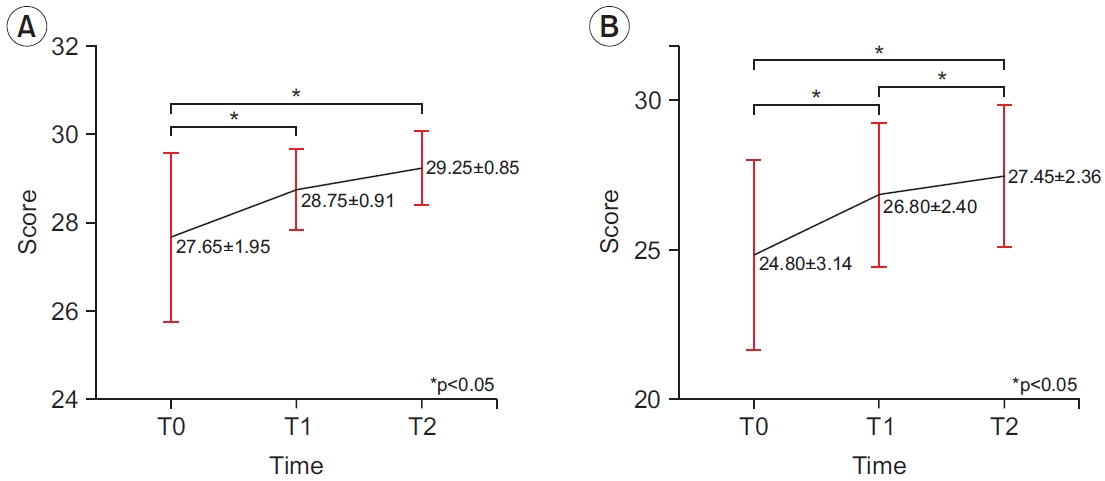
K-MMSE scores at T0, T1, and T2 were 27.65±1.95, 28.75±0.91, and 29.25±0.85 points, respectively, with statistically significant differences among the three time points (p<0.001). Mean K-MMSE scores increased by 1.10±1.97 from T0 to T1 (p=0.019), 1.60±1.76 from T0 to T2 (p=0.001), and 0.50±1.05 from T1 to T2 (p=0.057) (Fig. 3).
K-MoCA scores at T0, T1, and T2 were 24.80±3.14, 26.80±2.40, and 27.45±2.39 points, respectively, with statistically significant differences among the three time points (p<0.001). Mean K-MoCA scores increased by 2.00±2.43 from T0 to T1 (p=0. 003), 2.65±1.95 from T0 to T2 (p<0.001), and 0.65±1.27 from T1 to T2 (p=0.038) (Fig. 3).
Among individual items of the K-MMSE and K-MoCA, items requiring attention and memory showed improvements.
Safety evaluation
Safety evaluation was performed by examining adverse events, including perceived and objective symptoms and vital signs, based on participants’ self-reported data. All abnormal clinical symptoms that were not observed in the baseline measurements were classified as adverse events. Results were presented as the total number of adverse events, types of adverse events, the severity of adverse events, and the association between adverse events and the device. During the clinical trial period, two out of 20 participants showed adverse events, including urinary tract stone disease and ankle sprain. Both symptoms appeared after completion of the training, indicating no association between these symptoms and the training device, and the symptoms were mild enough for the affected participants to complete all training and evaluation procedures.
DISCUSSION
This clinical trial was conducted to examine the effects of integrated training by an integrated training device for strength and balance (SBT-120, Man&Tel Inc.) in conjunction with various rehabilitation games involving muscle strength, balance, and cognitive performance. The body balance performance was evaluated using various measurement tools such as BBS, FRT, and TUG showed significant improvements at T1 (immediately after the intervention) and T2 (4 weeks after the intervention) compared with T0 (baseline) (p<0.05). Post-training increase in strength was observed in all muscles, and cognitive performance, assessed by both K-MMSE and K-MoCA, also significantly improved after training.
Balance ability, assessed by the BBS, FRT, and TUG, improved after integrated training. Many factors affect body balance; muscle strength of the lower extremities is one of the major factors, and the lower extremity muscle strength decreases by 1%–2% every year as age increases [19]. Compared to middle-aged adults, older adults have a lower extremity muscle strength and hence impaired balance [20]. A study indicates that improvement in lower limb strength leads to increased lower extremity muscle strength, which in turn improves body balance, thus reducing fall risk [21]. Another study demonstrates the efficiency of concurrent training in improving muscle strength and balance [22]. Consistently, our study also showed that the indicators for balance were improved owing to the concurrent training of muscle strength and balance using our integrated training device. The games designed to increase lower extremity muscle strength were stamping and arrow games, which are closely associated with the exercise of the flexors, extensors, abductors, and adductors of the hip joint. Indeed, a conspicuous tendency to improve muscle strength related to the hip joint was observed in the lower extremity muscles. The improvement of muscle strength in the hip, knee, and ankle joints plays an important role in independent gait and balance recovery [21]; therefore, the integrated training device for strength and balance used in this study might help improve balance ability.
The results of the Nicholas MMT confirmed that the muscle strength in all muscles was improved after training compared to the baseline. The muscles that showed the greatest improvement were the flexors of the shoulder and hip joints. The muscles on the right side showed a greater improvement than those on the left side; the finding is inconsistent with the results of a study comparing the left- and right-side muscle strength after the same exercise, which reported the same exercise effect [23]. In the game using slings, participants use the extensors when pulling the slings, and the process of sustaining the strength of the sling to restore its original state is thought to help improve the strength of the flexor muscles. In addition, in the game using the IMU sensor, the vertical movement of the arms to maintain the arms at 90° is considered to help improve the flexor muscles of the shoulder joint. The hang glider game (with slings) is also considered effective in strengthening the lower extremity muscles by sustaining the tension of the slings to maintain balance by the opposite leg. In particular, in the game using the footpad (arrow game), the muscle of the ankle joint may be strengthened during the process of stepping on and detaching from the footpad. A decrease in the muscle strength of the hip and ankle joints has been demonstrated to be associated with the frequency of falls [24]. Thus, improving the muscle strength of the hip and ankle joints by training is assumed to improve the participants’ balance ability. The relatively high increase in muscle strength, although the training did not involve high-intensity exercise, might be due to the pretraining using the training mode of the investigated device, as well as regular exercise and physical activities, during the intervention period, which might improve self-efficacy with regard to the use of muscle strength [25] and increase muscle strength.
The K-MMSE and K-MoCA were used to evaluate participants’ cognitive performance, and it was found that both performance scores increased after training. The findings support the assumption that the four games played in conjunction with the investigated device improved cognitive performance. The games of the integrated device were designed to improve the attention, concentration, and memory of its users. In particular, the stamping game is considered to help improve cognitive performance because it requires the ability to solve the problem with a higher difficulty level in a shorter time window. Among individual items of the K-MMSE and K-MoCA, items requiring attention and memory showed improvements. A previous study reported that VR training improves memory and attention function in older adults [26]. This is in line with a previous study on the pathology of Alzheimer’s disease, which indicates that exercise prevents and delays cognitive decline in older adults and helps improve their cognitive ability [27]. Similarly, it has been reported that physical activity in older adults improves cognitive function and lowers the risk of dementia [28]. Taken together, these findings suggest that the six-week training with the investigated device helps participants increase muscle strength, as well as motor and cognitive abilities.
Our study showed that the training effect, especially improvement in balance, muscle strength, and cognitive performance, continued even 4 weeks after training, suggesting that the training effect of the integrated device might have been integrated into daily activities, and participants continued to be involved in more exercise than before due to the improvement of balance and muscle strength. This finding is consistent with that in a previous study on the training effect of video games in older adults, which indicates that the exercise effect persists even after a post-training break [29]. Recently, interest in sarcopenia, characterized by aging-related gradual loss of muscle performance and function, has increased because sarcopenia can cause cognitive impairment [30], heighten the risk of falls, and limit mobility [31]. Our findings indicate that the integrated device examined in the current study might have a positive effect on the strength, balance, and cognitive ability of patients with sarcopenia, and the effects on these patients should be investigated in future studies.
Studies have investigated VR-based balance training and muscle strength improvement training programs. A study determined the efficacy of a balance training program using Nintendo Wii Fit Plus and found that most participants had more pleasure and motivation in Nintendo Wii Fit Plus than in non-VR general intervention programs [6]. Notably, the present study also used VR game programs to engage users, and none of the participants appeared bored. Our findings suggest that the integrated training device for strength and balance investigated in this study provided older adults gratification and motivation throughout the training sessions using simple VR game programs.
The effects of devices similar to that used in the present study have been investigated previously. To improve muscle strength and movement of the upper extremity, exercise devices with VR [32] and training with elastic resistance [33] have been examined previously. The elastic resistance training has effects similar to those of the sling tasks used in the current study, and it has been shown that this training has similar effects compared to conventional resistance exercises [33]. Similar to the results of our study, previous studies observed improvements in upper limb muscle strength, and the device used in our study combined the advantages of VR devices and elastic resistance training. Likewise, improvements in muscle strength and balance in the lower extremity have been reported for a device similar to the footpad used in our study [34], resulting in improvements in lower limb muscle strength and balance. All these studies demonstrated effects similar to those of each component of the device used in the current study although, in prior studies, individual elements rather than an integrated device were used.
Studies on exercise equipment and programs are actively underway to increase the proportion of older adults who enjoy the health benefits of exercise. For example, studies on Tai Chi exercises have demonstrated a decrease in fall incidents through balance training [35] and an increase in cognitive performance [36] in older participants. Full-body vibration exercises have been reported to improve lower extremity muscle strength and balance and increase gait ability [37]. In addition, studies on balance training using the T-Bow [38] and Wobble board [39] have demonstrated improvements in balance control in older adults. In previous studies on VR rehabilitation devices, positive effects on cognitive function [26], balance [34], and strength [32] have been reported. In one study, VR dual-task training of cognition and balance effectively improved concentration, memory, and balance, but this study did not examine strength [40]. As far as we know, no study has yet been conducted to concurrently improve balance, muscle strength, and cognitive performance through a single intervention program. Conventional exercise programs or devices focus on only one or two of these functions. In contrast, the integrated training device for strength and balance used in this study can combine physical training with game programs to enhance balance, muscle strength, and cognitive performance. Additionally, multifaceted evaluations of each factor were performed in this study using a variety of scales to quantitatively measure the improvement in cognitive ability and muscle strength and balance, as well as the persistence of the exercise effect, which is also a distinct feature analyzed in this study compared with previous studies.
This study has several limitations. First, it was a small-scale single-group study with no control group. Therefore, to determine the efficacy of SBT-120 more accurately, a follow-up study with larger sample size is necessary to yield more definitive results. Second, there was no exact numerical indicator of the tension exerted on the sling, and the user’s maximum force could not be taken into account. If the tension of the sling could be measured and adjusted to the user’s individual muscle strength, it would have been possible to further increase the training effect. Third, the difficulty levels of the games were uniformly set to three levels without gradually adjusting the difficulty level based on individual cognitive ability. Further studies are needed to confirm our present finding by adjusting the game difficulty level based on individual cognitive abilities. Fourth, regarding cognitive performance, there was an improvement in K-MMSE and K-MoCA, but the learning effect was not considered. Fifth, among the evaluation tools used in this paper, there may be subjectivity biases in those evaluated by a rater. Finally, participants in this study were all healthy older adults. Further studies are necessary to clarify the clinical implications of the investigated device in patients with impaired balance, muscle strength, and cognitive ability.
In conclusion, the integrated training device for strength and balance investigated in this study could serve as a useful device for concurrently increasing muscle strength, balance, and cognitive performance in older adults. This training device can encourage older adults to receive training by combining various exercise programs featuring challenging balance and cognitive tasks, which provide motivation to practice its systematic exercise programs, and thus enhancing their quality of life.