INTRODUCTION
Spinal cord injury (SCI) is one of the major insults to the central nervous system that results in persisting physical and psychological sequelae, thereby incurring tremendous socioeconomic costs related to health care treatment, rehabilitation, and loss of productivity [1-4]. Therefore, extensive efforts for predicting and preventing SCI should be made to improve national health and welfare. Educational programs that are designed based on epidemiologic studies have shown to be successful in reducing the incidence of traumatic SCI [5-8]. In the United States, epidemiologic changes in age, sex, and completeness of injury of SCI are continuously being monitored by the National Spinal Cord Injury Statistical Center (NSCISC), and a gradual increase in the prevalence of the people with old age, female sex, and incomplete injury has been reported [9-12]. In Asia, only Japan and Taiwan are counting and registering traumatic SCI people in the perspective of epidemiology. Other Asian countries, including Korea, do not take the same approach [13]. Particularly, in Korea, people with SCI are being counted as having “physical disability” and clustered together with other disabilities; thus, the exact incidence of SCI can only be assumed indirectly [14]. Some of the most recent studies in Korea that analysed national demographic data specific to SCI were those by Park et al. [15], Shin et al. [16], and by the National Rehabilitation Center [17]. Park et al. [15] reported traffic accidents as the most common cause of traumatic SCI, accounting for 57.6%, and falls as the second most common cause, accounting for 26.4% in 1999. However, the study by the National Rehabilitation Center in 2014 [17] showed that the percentage of SCI caused by traffic accidents had decreased from 64% in 1994–2000 to 45% in 2008–2014. The proportion of falls had risen from 23% to 43% during the same time intervals, implying a change in trends regarding the etiology of traumatic SCI.
There are many explanations and hypotheses in interpreting the changes in SCI epidemiology worldwide, and understanding each country’s demographic characteristics and cultural specificity in connection with etiology is important in interpretation. For example, falls account for 63.0% of SCI in Bangladesh, which is a developing Asian country with a low-income economy and a small urban population. Those injuries mostly occur among those aged between 10 years and 40 years and are mainly attributed to falling from trees or carrying heavy objects on the head. Meanwhile, in eastern Canada, which is a developed country with a high-income economy and a large urban population, the mean age at the time of SCI was 55.4 years, and falls accounted for only 19.1% of SCI etiology. However, falls were the leading cause of SCI in the elderly (i.e., age ≥60 years), accounting for 47% [18].
One of the most remarkable demographic characteristics of Korea is rapid aging of population, and this is occurring in many developed nations including those in Europe [19,20]. Data from Statistics Korea show that in 2018, 14.3% of the population were aged ≥65 years, and this proportion is projected to increase to 35.9% by 2050 and to 41.0% by 2060 [21,22].
On the other hand, one of other characteristics of Korean population is high prevalence of ossification of posterior longitudinal ligament (OPLL), which is thought to be related to incurring cervical SCI with minor trauma [23-25]. OPLL is pathological calcification of posterior longitudinal ligament, which occurs more frequently in Asian population than other races [26] and most commonly at the cervical spine [27]. Depending on the size, OPLL can results in the spinal canal narrowing and more importantly, compression of the spinal cord and trauma-induced sudden onset myelopathy. The mainstay treatment of OPLL is surgical decompression, including corpectomy, laminectomy, and combined fusion [27].
This study aimed to investigate the effect of demographic changes on SCI epidemiology in Korea with cross-sectional data of single university hospital. We hypothesized that an aging population might present more injuries caused by minor traumas such as low falls including slip-down and tripping over even in level ground or in the stairs, as in other developed countries. We also hypothesized that increase in mean age of SCI people might be related to more comorbidities of degenerative diseases such as OPLL, which contributes to SCI. To determine the impact of population aging on changes in SCI etiology, we separated falls into two categories, namely, high-energy trauma and low-energy trauma, by separately calculating the high falls (falling off) and low falls (tripping over).
MATERIALS AND METHODS
Study design and subjects
This was a descriptive cross-sectional study of individuals with SCI from traumatic or non-traumatic causes who were hospitalized for comprehensive rehabilitation to a dedicated hospital between January 2012 and June 2018. Data on demographic, injury, and medical characteristics were obtained from hospital admission records. This study was approved by Inje University Ilsan Paik Hospital Institutional Review Board (No. 2020-03-027). SCI was defined as the event of a traumatic or non-traumatic lesion of neural elements in the spinal canal that resulted in temporary or permanent sensory and/or motor deficit [28].
Descriptive analyses of SCI are suggested with stratification by key demographic characteristics and SCI-specific characteristics (e.g., sex, age at injury, American Spinal Injury Association Impairment Scale [AIS] score at admission and discharge, SCI type, and etiology) according to the International Spinal Cord Society guidelines, where possible [29].
Categorization of falls
Falls were categorized into low (<1 m) or high falls (≥1 m) based on available information on cause of injury in the medical records [28]. A 1-m cutoff for classifying the level of falls was chosen to facilitate comparison with previous reports in the literature and with reference to the World Health Organization’s (WHO’s) International Perspectives on SCI report. The WHO report categorized falls into 4 different patterns: (1) falls on the same level, (2) falls from heights of <1 m, (3) falls from heights of ≥1 m, and (4) being struck by a falling object [30]. We classified categories 1 and 2 as low fall (tripping over), and 3 as high fall (falling off). There was no case for category 4 in this study.
Statistical analysis
Descriptive statistics (mean, standard deviation, frequency, ratio, and percentage) were used to describe the clinicodemographic characteristics of the study participants across injury etiologies. Student t-test and chi-square test, as appropriate, were used to assess the differences between the etiology groups at a statistical significance level of 0.05. All analyses were performed using the IBM Statistical Package for the Social Sciences, software version 22.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Epidemiology and demographics
In total, 221 cases of SCI were included in the study. Of these, 161 were traumatic and 60 were non-traumatic. In the traumatic SCI group, 134 (83.2%) were men and 34 (16.8%) were women; in the non-traumatic SCI group, 27 (56.7%) were men and 26 (43.3%) were women. The proportion of male patients was noticeably higher in the traumatic SCI group at 4.96:1 than in the non-traumatic SCI group at 1.30:1. The mean age of the overall cohort was 52.8±17.9 years, and that of the traumatic and the non-traumatic SCI groups were 49.8±18.0 and 60.7±15.2 years, respectively. The patient characteristics are shown in Table 1. The proportion of the 40–49 year age group was the highest among overall patients (19.0%), and majority (21.1%) of patients in the traumatic SCI group were also aged 40–49 years. Meanwhile, majority (26.7%) of patients in the non-traumatic SCI group were aged 70–79 years.
Etiology
With respect to etiology, falling off was the most common cause of traumatic SCI (n=60/161, 37.3%), followed by motor vehicle crashes (MVC) (n=57, 35.4%) (Table 2). Categorizing tripping over and falling off (n=31, 19.3%) together as falls, it becomes a more dominant cause of traumatic SCI, accounting for 56.5%. The age distribution according to the detailed trauma etiology is shown in Table 2. The most common cause of SCI varied in each age group. In the 10–19, 20–29, and 50–59 years age group, falling off was the most common cause of traumatic SCI, accounting for 54.5%, 63.6%, and 46.2%, respectively. Meanwhile, in those aged 60 years or older, tripping over was the leading cause of traumatic SCI, accounting for 37.0%, 40.9%, and 80.0% in the 60–69, 70–79, and 80–89 years age groups, respectively. The mean age of each traumatic etiology was also distinct from each other. Particularly, patients who were injured by tripping over showed a significantly higher mean age of 62.9±16.9 years compared to patients with other etiologies (p<0.001).
The mean age and AIS score and the detailed number of cases of non-traumatic etiology are shown in Table 3. The most common cause of non-traumatic SCI was neoplasm, accounting for 35.0%. The mean age of each etiology was mostly over 60 years, except for infectious disease and other non-traumatic causes, which was at 59.1 and 56.6 years, respectively. There were only two patients who presented complete injury (AIS-A), while the other 58 patients were incompletely injured by non-traumatic causes.
Type of disability and severity of injury
The types of disabilities and severity of injury caused by SCI are detailed in Table 2. The majority (47.8%) of traumatic SCI patients presented incomplete tetraplegia, except patients who were injured by falling off. Most (74.2%) of the patients who were injured by tripping over presented incomplete tetraplegia. Non-traumatic causes of SCI most commonly resulted in incomplete paraplegia (58.3%) followed by incomplete tetraplegia (38.3%).
Prevalence of OPLL in traumatic SCI patients
Table 4 shows the number of patients with OPLL in the traumatic SCI group. In total, 42 patients (26.1%) were found to have underlying OPLL. The prevalence of OPLL in patients who were injured by tripping over was high at 64.5% (20/31 cases). Among the traumatic SCI patients with OPLL, the level of OPLL and neurological level of injury matched each other in 92.9% (39/42 cases).
DISCUSSION
This study investigated the epidemiologic and demographic characteristics of patients with SCI who were admitted to rehabilitation unit of a university hospital in South Korea. We found a significantly higher proportion of male patients than female patients. Specifically, 76.0% of the patients were men, with a male-to-female ratio of 3.17:1 (168:53). This result is similar to that of one of the latest Korean epidemiologic study by Shin et al. in 2013, which showed that 74.1% of patients with all-cause SCI were men, with a male-to-female ratio of 2.86:1 [16]. This sex imbalance was more profound in traumatic SCI patients, with a male-to-female ratio of 4.96:1 (134:27), which is consistent with or more significant than that in previous epidemiologic studies in Korea [14,16,17]. This tendency of dominance of male cases in traumatic SCI is also consistent with previous epidemiologic studies in other developed countries [28,31]. Meanwhile, non-traumatic SCI showed smaller difference in the sex ratio at 1.30:1 (34 males, 26 females) in our study, which is closely consistent (1.47:1) with recent study by Shin et al. [16].
With respect to the etiology of traumatic SCI, our study showed that falls, counting low and high falls together, was the single most common cause, accounting for 56.5% (n=91) of all traumatic causes, followed by MVCs at 35.4% (n=57). The dominance of falls as a cause of traumatic SCI in our study is consistent with the trend of recent studies on traumatic SCI epidemiology [9,28,31,32]. This trend of changes in etiology is relatively recent finding in Korea. From 1987–1996 to 2004–2008, the proportion of MVC and falls both increased from 57.6%, 26.4% to 60.3%, 33.9%, relatively [16]. However, comparing the etiology from 2004 to 2014, the proportion of MVC decreased from 64% to 45% and falls increased from 23% to 43% [17].
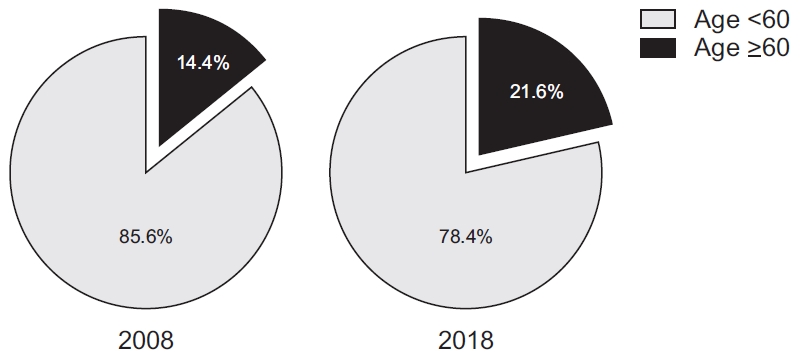
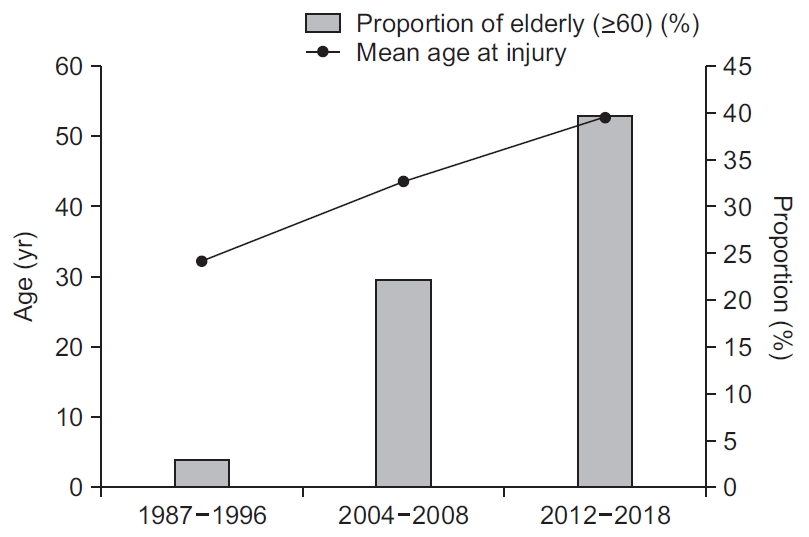
It is also assumed that the older mean age of the patients at the onset of trauma in our study might have contributed to this result. According to the population data from Statistics Korea, the proportion of people older than 60 increased from 14.4% to 21.6% between 2008 and 2018 [33] (Fig. 1). Comparing our study results with the previous study of Shin et al. [16], the proportion of people older than 60 among traumatic SCI patients increased from 20.0% to 33.5%, from 2004–2008 to 2012–2018. Changes in the mean age at overall SCI and proportion of the patients older than 60 are shown in Fig. 2. Shin et al. [16] reported that falls was the most common cause of injury in people older than 60 years, with falls accounting for 54.2% of all traumatic causes in this age group. In our study the proportion of falls was highest among all causes of traumatic SCI in the patients aged 60 years or older, accounting for 68.5%. Similar trend is observed in other developed countries. In the United States, falls are the leading cause of SCI among persons aged over 60 years accounting for 55.8% [12]; in Norway, falls accounted for 65% of all injuries in persons older than 60 years [9,31]. In the United States, the mean age at SCI onset tended to be consistent and then gradually increased. In the 1970s, the mean age was 28.7 years, but it increased to 37.6 years in 2000–2004 and to 43.1 years in 2015–2019 showing increasing ages in all causes of SCI [12]. In Korea, the mean age at SCI onset was 32.3 years in 1985 and increased to 43.6 years in 1999. In our study, the mean age at SCI was 52.8 years, and 39.82% of the overall SCI patients were aged 60 years or older.
Our study counted low fall and high fall separately to place them into low-energy trauma and high-energy categories. In total, 60 and 31cases of traumatic SCI were attributed to high fall and low fall, respectively. Among the 54 patients aged over 60 years, 14 patients were injured from high fall, accounting for 25.9% of all traumatic causes in this age group. Twenty-three patients in the same age group were injured by low fall, accounting for 42.6% of all traumatic causes in this age group. A similar tendency is also found in the United States. Compared with other age groups, the elderly had the highest frequency of low falls on the same level, from the stairs, and slipping and stumbling [32]. The incidence of fall-related traumatic SCIs appeared to be age dependent, particularly for low fall injuries. In traumatic SCIs, the proportion of SCI from falls increased with age; 14.4%, 38.7%, 55.8% in 0–45, 46–60, over 61 age groups, respectively [12].
In this study, we investigated the prevalence of OPLL in SCI patients, which is a common comorbidity for Asians. OPLL contributes to the occurrence of low-energy traumatic SCI, particularly, cervical cord injury when low fall accidents happen. Among the 31 patients with traumatic SCI who experienced low fall injuries, 20 (64.5%) had underlying OPLL. This proportion is much higher than the 0.6%–4.6% prevalence of incidental finding in the normal population in previous national studies [23,25,34]. In those studies, OPLL was prevalent in 16.9% of men aged over 65 years, which is higher than that in younger people, but still far lower than among the patients who experienced low falls in our study. This tendency of higher prevalence of OPLL in older patients supports our findings that show a correlation between higher mean age of traumatic SCI patients and incomplete cervical cord injury caused by low fall event.
Among non-traumatic etiologies, neoplasm was the single most common cause of SCI, accounting for 35.0%, followed by demyelinating disease and infectious disease as the second most common causes (16.7% each). Vascular disease accounted for 10% and degenerative disease followed at 8.3%. Other causes including herniated vertebral disc, spinal stenosis accounted for 13.3% of non-traumatic SCI.
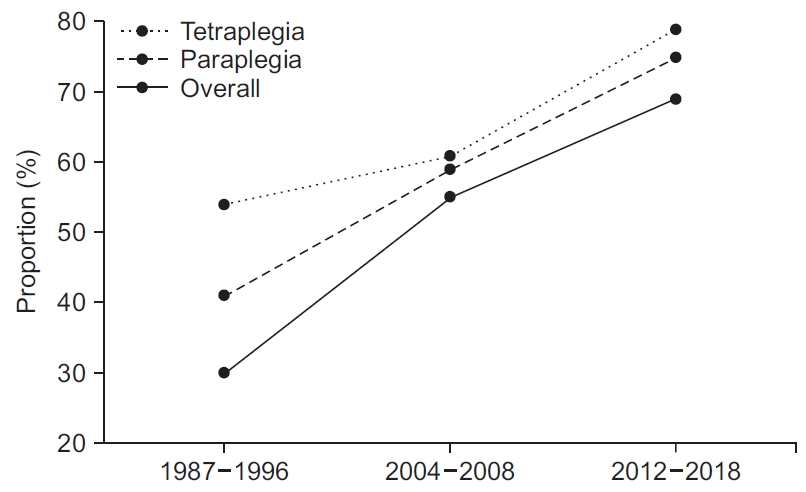
With respect to disability types and severity of injury, the epidemiologic study by Shin et al. [16] in 2013 showed incomplete tetraplegia as the most common type, accounting for 36.9% of all SCI. According to annual reports of NSCISC [12] and as Jain et al. [35] suggest, the proportion of cervical spinal cord injury and incomplete injury has increased gradually in United States. In our study, 127 (54.3%) patients had tetraplegia, and only 27 (21.3%) among them presented complete injury. Gradual increase in the proportion of incomplete injury from 1987–1996 to 2012–2018 according to previous study and our study results is shown in Fig. 3 [16]. A notably low proportion of complete injury might be attributed to not only developments in prompt medical and surgical management after SCI, but also the increase in low-energy trauma injuries. In our study, the mean age of patients was higher than that in previous studies, and incomplete tetraplegia was the most common result after low-energy trauma. Among 31 patients who were injured by low fall, 27 (87.1%) had tetraplegia, and only 4 among them presented complete injury.
There are several limitations in this study. The data source for this study was limited to one university hospital and is not population based. Therefore, our study results might not be generalizable to the overall population of people with SCI in Korea. Also, we could only acquire information from the patients who were admitted or transferred to the rehabilitation medicine department of our hospital. Thus, we could not evaluate SCI patients who died or were discharged before transferring to our department. This might result in underestimation of the fatal SCI or less severe SCI. In addition, we could only check the patients’ AIS upon admission or when they were transferred to our department. Therefore, the timing of evaluation of severity and type of SCI varied, and this which could have influenced the severity of injury itself. Lastly, we did not analyse specific types of OPLL in the traumatic SCI patients. It would be meaningful to specify the type of OPLL in correlation with the SCI in further study. Despite these limitations, our study remains valuable because to our best knowledge, this is the latest study that reports the epidemiology and etiology of SCI in Korea.
In conclusion, this study demonstrates the cross-sectional analysis of the clinicodemographic characteristics of SCI patients in a university hospital in South Korea and showed its similarity with that of other developed, aging countries in Europe and North America. The epidemiology of SCI in Korea might be characterized by high mean age at time of injury and dominance of falls, especially low falls, as a cause of traumatic SCI.