INTRODUCTION
Steroids are being used effectively for the treatment of a variety of musculoskeletal disorders, including osteoarthritis, tendonitis, myofascial pain syndrome, and trigger fingers [1,2]. They are especially useful for shoulder or spinal diseases, mainly for the treatment of shoulder pain caused by rotator cuff disease or adhesive capsulitis and spinal pain caused by herniated nucleus pulposus (HNP) and spinal stenosis [1-7]. Steroids are useful for treating severe pain that requires surgical treatment in patients who cannot undergo surgery due to medical complications or other problems. However, steroid use is accompanied by various side effects such as fever, facial flushing, nausea, and fatigue. One typical side effect of steroid injection is an increase in blood glucose level [8-12].
Steroid use can inhibit the function of the hypothalamicŌĆōpituitaryŌĆōadrenal (HPA) axis, rendering patients vulnerable to adrenal insufficiency and with blood glucose levels that are difficult to control [13,14]. It can also lower the function of glucose metabolism and stimulate gluconeogenesis, thereby increasing blood glucose level and resistance to insulin [15].
Patients with diabetes mellitus (DM) are more vulnerable to vascular injury, joint and disk disorders, and degenerative changes, and have a higher prevalence of shoulder and spinal diseases than patients without DM [16-18]. The active use of steroids in clinical practice is limited, because elevated blood glucose and associated risks are increased in patients with DM after steroid use. Recently, several studies have investigated blood glucose level elevation after steroid injection in specific areas such as wrist, finger, shoulder, and knee [10,19-24]. Although previous studies have shown blood glucose level elevation after steroid injection, the duration of blood glucose level elevation and whether blood glucose level elevation is higher in patients with poor blood glucose control, such as those with high HbA1c or taking insulin, remain controversial [23,25,26].
Therefore, the aim of this study was to investigate the duration of blood glucose level elevation and the factors affecting the degree of blood glucose elevation after steroid injection in patients with type 2 DM. We hypothesized that patients with poor blood glucose control, such as patients with high HbA1c levels or those taking insulin, would have greater blood glucose level elevation.
MATERIALS AND METHODS
Participants
Between August 2017 and December 2018, we retrospectively enrolled 82 patients with type 2 DM who had been admitted to our hospital, were using diabetes medication or insulin, and had undergone steroid injection for joint pain. This study was approved by the Institutional Review Board of Gwangju Veterans Hospital (No. 2019-2-1). The informed consent was waived.
The exclusion criteria were as follows: (1) patients younger than 18 years; (2) patients who had received steroid injection in the previous 3 months; (3) patients currently taking oral steroids; (4) patients with blood coagulation disorders or those in whom steroids were contraindicated or those with infections or systemic disease; (5) patients who had not monitored HbA1c level before injection or those who did not monitor blood glucose levels before or after injection.
Of the 61 patients who were not excluded, 51 patients with shoulder pain caused by adhesive capsulitis or rotator cuff disease or with back pain due to spinal stenosis or HNP were included in this study (Fig. 1). Age, sex, DM duration, body mass index (BMI), HbA1c levels during 3 months prior to injection, hypertension (HTN) presence, insulin usage, injection site, and steroid dose were investigated as factors that could affect blood glucose levels after steroid injection (Table 1).
Injection protocol
Based on medical records, patients with shoulder pain were injected with triamcinolone 20 mg or triamcinolone 40 mg at the subacromial subdeltoid bursa or intraarticular area according to their symptoms and lesions. Patients with spine problems were treated with transforaminal epidural injection and/or medial branch blocks depending on their symptoms and lesions. They were injected with dexamethasone 10 mg or dexamethasone 20 mg plus triamcinolone 40 mg. To compare the change in blood glucose according to steroid dose, triamcinolone 40 mg and dexamethasone 7.5 mg were studied as dose equivalent [27,28].
Outcome measures
We referred to the confirmed measured HbA1c levels during the previous 3 months before steroid injection and blood glucose levels during hospitalization. The mean of fasting blood sugar (FBS) levels for 1 week prior to steroid injection was considered the baseline blood glucose level. FBS level was checked for 14 days after steroid injection and compared with baseline. Patients used existing medications and insulin as usual after steroid injection. Based on these data, we investigated whether steroid injection affected blood glucose level elevation. We categorized patients into two groups based on HbA1c 7%. We also categorized patients into two groups based on whether they were being treated with insulin. We examined differences in blood glucose level changes between HbA1c >7% and HbA1c Ōēż7% groups and between insulin and non-insulin groups. We also examined various factors that might have affected blood glucose levels.
Statistical analysis
Data are presented as mean┬▒standard deviation. All statistical analyses were conducted using SPSS version 22.0 (IBM, Armonk, NY, USA). FBS after steroid injection over time were evaluated using repeated measures of ANOVA. We compared the degree of FBS level elevation 1 day after injection between the HbA1c >7% and HbA1c Ōēż7% groups and between the insulin and non-insulin groups using the Student t-test. Multiple regression analysis was used to confirm the relationships between patientŌĆÖs factors and the degree of FBS level elevation 1 day after injection with respect to baseline FBS. A p-value of less than 0.05 was considered statistically significant.
RESULTS
Blood glucose change after steroid injection
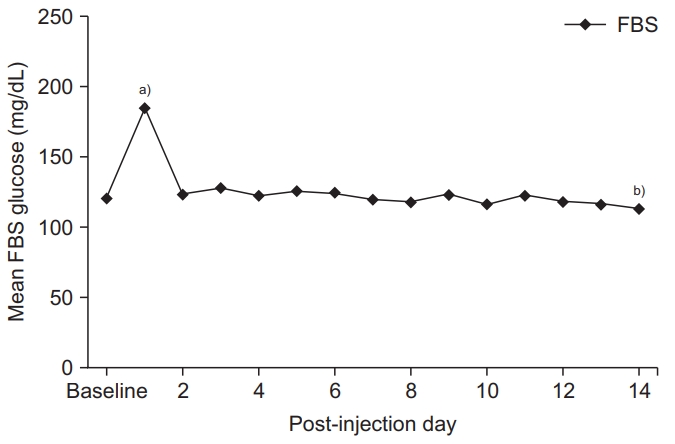
FBS after steroid injection over time was statistically significant using repeated measures of ANOVA (p=0.000) (Fig. 2). One day after steroid injection in all the patients, blood glucose levels had significantly increased by 64.0┬▒29.4 mg/dL compared with baseline blood glucose (p=0.012). However, at 2 days after injection, blood glucose levels reverted to baseline levels, showing no significant increase with respect to the baseline blood glucose levels (p=0.333) (Fig. 2).
Factors affecting blood glucose elevation
Blood glucose level was significantly elevated 1 day after steroid injection compared to baseline blood glucose, but not 2 days after injection, so we analyzed the relationships between the degree of blood glucose increase 1 day after steroid injection and the various factors.
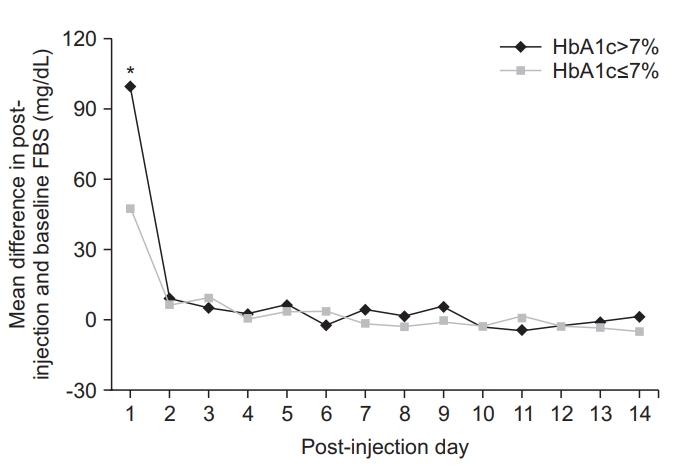
Both HbA1c >7% (p=0.019) and HbA1c Ōēż7% (p=0.027) groups had a statistically significant increase in blood glucose 1 day after steroid injection. There was also a significant difference in the increase in blood glucose level between the two groups (p=0.011). In the HbA1c >7% group, blood glucose level was increased by 99.4┬▒30.7 mg/dL with respect to baseline. In the HbA1c Ōēż7% group, blood glucose was increased by 47.6┬▒10.1 mg/dL with respect to baseline. However, there was no significant difference in the decrease in blood glucose levels between the two groups because blood glucose levels had declined to baseline 2 days after steroid injection (p= 0.142) (Fig. 3).
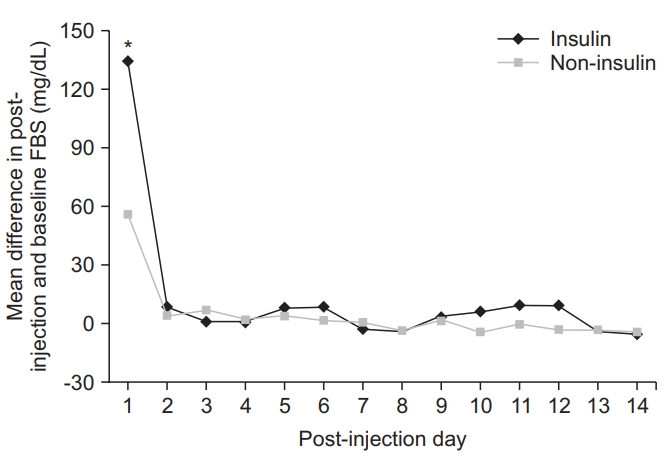
Both the insulin group (p=0.022) and non-insulin group (p=0.035) showed a statistically significant increase in blood glucose levels 1 day after steroid injection. A significant difference in the increase in blood glucose levels was observed between the two groups (p=0.024). In the insulin group, blood glucose level was increased by 134.5┬▒37.6 mg/dL with respect to baseline. In the noninsulin group, blood glucose was increased by 56.2┬▒19.2 mg/dL with respect to baseline. However, no significant difference in decrease in blood glucose level was observed between the two groups because blood glucose levels had declined to baseline 2 days after steroid injection (p=0.213) (Fig. 4).
Among various factors, we found that the higher the HbA1c level before injection, the more significant the blood glucose increase after injection (r=0.419, p=0.003). However, multiple regression analysis revealed that age, sex, DM duration, BMI, HTN presence, insulin use, injection site, or steroid dose did not significantly affect blood glucose after steroid injection (p>0.05) (Table 2).
During the study, side effects, such as diabetic ketoacidosis or hyperosmolar nonketotic coma as hyperglycemic complications resulting from steroid injection, were not observed.
DISCUSSION
The aim of this study was to investigate the duration of blood glucose level elevation after steroid injection in patients with type 2 DM and whether associated factors and poor blood glucose control play a role in the elevation of blood glucose levels. A total of 82 patients were retrospectively reviewed. Of 61 patients who met the inclusion criteria, 51 patients who had received steroid injections in the shoulder or spine were enrolled in this study. Patients with steroid injection in the shoulder or spine were enrolled because we assume the effect of the injection on blood glucose levels can be more precisely studied when the injection is administered to a large joint. Conversely, we considered that small joints, such as the wrist and those of the fingers, are usually injected with small volumes of steroid, making it difficult to precisely examine any side effects of the injected steroid [29].
After steroid injection, blood glucose levels were significantly elevated for 1 day but decreased to baseline levels after 2 days. Clinically, HbA1c levels have been reported to be significant in terms of glycemic control for the previous 3 months and response to DM treatment [19,30]. Commonly, patients with HbA1c levels exceeding 6.5% are diagnosed with DM. Previous studies have recommended that HbA1c levels be maintained below 7%, because the risk of various complications due to DM are increased if HbA1c levels exceed 7% [31]. Therefore, we categorized participants into two groups based on HbA1c (Ōēż7% or >7%). Participants were also categorized into two groups according to insulin treatment. Blood glucose levels were more significantly increased one day after steroid injection in the HbA1c >7% and insulin groups, than in the HbA1c Ōēż7% and non-insulin groups, respectively, which is congruous with the results of Aleem et al. [22]. When patients were compared on the basis of HbA1c 6.5%, no significant differences were noted between the two groups in the degree of blood glucose level elevation 1 day after steroid injection. A few previous studies on the differences in blood glucose levels between the two groups according to HbA1C 7% level and insulin were identified, but no study has reported whether HbA1c levels or insulin dependence are associated with blood glucose level elevation. In this study, multiple regression analysis showed that HbA1c level was associated with blood glucose level elevation, whereas insulin use was not associated with such elevation. Because multiple regression analysis includes the effects between factors, it is a more meaningful method in analyzing the factors that may affect blood glucose elevation. This indicates that the degree of usual blood glucose control rather than insulin dependence is related to blood glucose level elevation after steroid injection.
Several studies have investigated blood glucose level changes after steroid injection. Wang and Hutchinson [20] reported that after injecting 10 mg of methylprednisolone into the trigger finger of 18 patients, blood glucose level was significantly increased for 1 day after injection but returned to the baseline level on the second day. Stepan et al. [10] have reported that after 20ŌĆō120 mg of methylprednisolone was injected into the hand and wrist of 40 patients, blood glucose level was significantly elevated for 2 days after injection but returned to baseline on the third day. These results are consistent with our results, showing that blood glucose levels were significantly elevated for 1 day after steroid injection but returned to baseline after 2 days, and showed no significant increase with respect to the baseline level. After steroid injection, extrinsic steroids inhibit the function of the HPA axis, rendering patients vulnerable to adrenal insufficiency and with blood glucose levels that are difficult to control [13,14]. Other studies have shown that more doses of steroids increase the risk and duration of blood glucose elevation, which has led to changes in existing diabetes treatments [26,32,33]. These results differ from those of our study, which showed a significant increase in blood glucose for 1 day after steroid injection. Because only a single and limited dose of steroid was injection in our study, it is possible that the steroid dose used in our study did not have a significant effect on HPA axis inhibition seen in patients with diabetes.
Choudhry et al. [34] performed a systematic review of literature related to steroid injection in DM patients. They reported that patients exhibited elevation of up to 500 mg/dL in blood glucose levels after steroid injection. However, no patients had severe complications such as diabetic ketoacidosis or hyperosmolar nonketotic coma. The results of their study were consistent with those of our study in which diabetic ketoacidosis or hyperosmolar nonketotic coma were not observed, although 5 patients exhibited elevation of up to 350 mg/dL in blood glucose levels with respect to the baseline glucose levels, after steroid injection.
This study has some limitations. First, although it was a retrospective study, the sample size was relatively small. However, it is a retrospective study based on blood glucose records. Therefore, blood glucose results were accurate. In previous prospective studies that were not based on medical records, recall bias may have been present, because patientsŌĆÖ measured blood glucose results and data collection were based on patient memory. Second, as all the patients had type 2 DM, there were no comparisons made between type 1 DM and type 2 DM or between non-DM and type 2 DM. Third, most patients were over 60 years old and male. Thus, we were unable to fully control the variables. Fourth, we did not study the effects of common diabetic complications, such as chronic kidney disease, retinopathy, and sarcopenia, on blood glucose level elevation. Future studies considering these aspects are required. Fifth, although particle steroids may have a longer tissue effect duration, which may affect glucose metabolism, we did not study the changes in blood glucose that may be caused by particle differences between dexamethasone and triamcinolone. Sixth, we did not examine whether steroid injection has long-term effects on blood glucose level elevation. HbA1c levels have been reported to be significant in terms of the status of glycemic control for 3 months [19,30]. Therefore, HbA1c is a reliable method to understand the effect on long-term blood glucose control after steroid injection. However, because it was a retrospective study, we could not periodically assess HbA1c after steroid injection nor could we control for re-injection or changes in diabetes treatment modality after steroid injection.
Active steroid use in patients with type 2 DM has been challenging because the duration for which blood glucose levels remain elevated is unclear. However, this study showed that blood glucose levels increased for up to 1 day after steroid injection and returned to the baseline level on the second day. Among various factors, HbA1c level affected the extent of increase in blood glucose levels. Patients who had poor usual blood glucose control had higher blood glucose levels after steroid injection. Based on results of this study, steroid injection in should be administered more carefully in patients with higher HbA1c levels. As blood glucose levels increase for up to 1 day after steroid injection, steroids can be safely used if blood glucose levels are regularly monitored and managed during this transient elevation period.