INTRODUCTION
Post-stroke memory impairment is the second-most common cause of dementia. Its prevalence is 11%–31% in non-demented patients 1 year after stroke [1]. Post-stroke impairment decreases the quality of life of a patient. It may even make it difficult for patients to return to normal life.
The limbic system is deeply responsible for the function of memory and behavior. The Papez circuit is composed of limbic gray and white matter. The circuit begins in the hippocampus, which is connected to the mammillary body via the fornix. The mammillary body is then connected to the anterior thalamic nuclei via the mammillothalamic tract (MTT). Next, the anterior thalamus is connected to the cingulum via the thalamocortical tract (TCT). The cingulum runs down to the end of the entorhinal cortex which projects to the hippocampus [2]. Previous studies with conventional magnetic resonance imaging (MRI) have reported that lesions to the Papez circuit such as in the thalamus or hippocampus are correlated with memory impairment [2,3]. However, these conventional images are unable to show whether inter-connected pathways of the Papez circuit are injured in the limbic system three-dimensionally. Recently, diffusion tensor tractography (DTT) has allowed for the Papez circuit to be visualized three-dimensionally and analyzed in a quantitative manner [4]. Furthermore, memory impairment in patients with brain injury has been shown to be associated with lesions on the entire neural tract in the Papez circuit three-dimensionally [5-9]. However, to date, no study has reported on the association between memory impairment and the integrity of the entire tract of the Papez circuit after multiple cerebral infarcts. Therefore, the objective of this study was to clarify the mechanism of memory impairment in a patient with concurrent thalamic and hippocampal infarctions. All four neural tracts related to the Papez circuit were reconstructed using DTT. Our findings may contribute to the elucidation of the mechanisms involved in the memory impairment in patients with cerebral infarction.
CASE REPORT
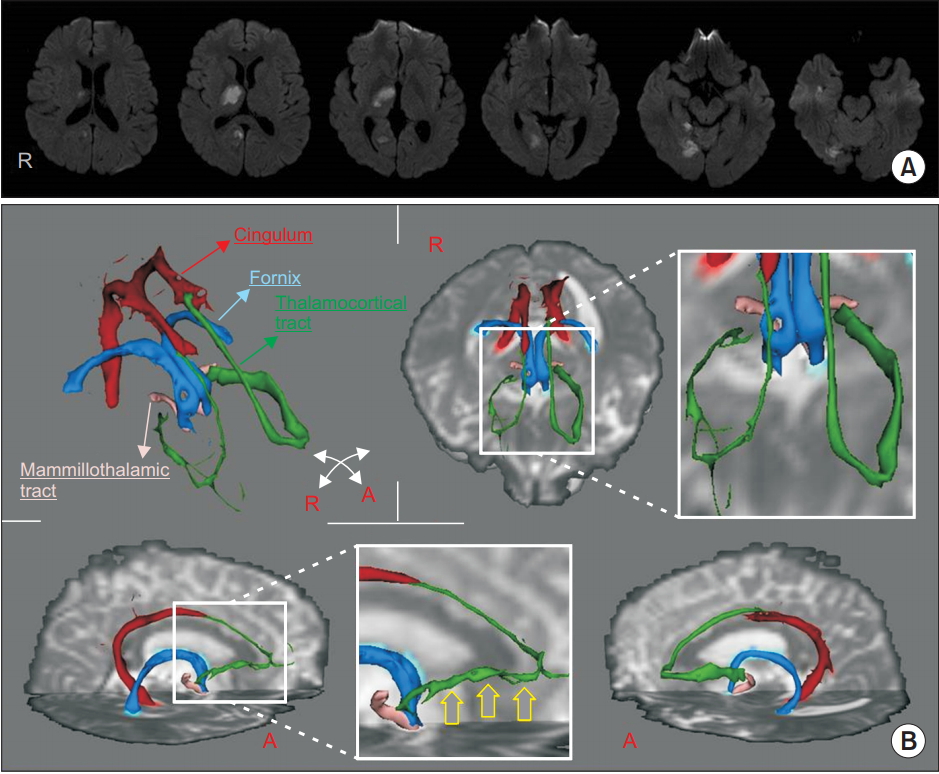
A 20-year-old male soldier abruptly experienced motor weakness 3 days before being referred to our department through the Department of Neurology. Initial diffusion brain MRI showed multiple cerebral infarcts on the thalamus, hippocampus, and fusiform areas (Fig. 1A). Upon admission, a physical examination revealed that the motor power of the left extremity was severely decreased. In a manual muscle test, the upper and lower extremities of the left extremity scored 4/5. Other neurological examinations were normal. The patient could only walk with supervision. A month after the onset of weakness, he was able to return to normal life activities but still complained of memory impairment. We studied the cause of memory impairment with probabilistic DTT at 32 days after the onset. Neuropsychological evaluation was performed at 43 days after the onset. Diffusionweighted imaging data were analyzed using the Oxford Centre for Functional Magnetic Resonance Imaging of the Brain (FMRIB) Software Library. Fiber tracking was performed with the probabilistic tractography method based on a multifiber model. Tractography routines were implemented in FMRIB (diffusion for 5,000 streamline samples at 0.5 mm step length and curvature threshold of 0.2 corresponding to a minimum angle of 80°). The neural tracts of the Papez circuit were reconstructed [6]. The integrity of the fornix, cingulum, and MTT was wellmaintained on both hemispheres in a three-dimensional view. Although the TCT showed symmetrical appearance between both hemispheres, the right TCT between the anterior thalamic nuclei and the cingulate gyrus was shown to be thinner compared to the left TCT (Fig. 1B). Neuropsychological scores revealed the following results. First, the verbal memory scores for short-term, delay, and recognition were in the 6.81, 33.72, and 72.24 percentiles, respectively. The visual memory scores for short-term, delay, and recognition were in the 24.83, 12.51, and 64.43 percentiles, respectively. Second, his Wechsler Adult Intelligence Scale score was 103. Third, the frontal and executive functions were normal and the scores for visuospatial and attention tests were in the 92.22 and 88.10 percentiles, respectively. These findings indicated memory impairment (mainly short-term verbal memory).
DISCUSSION
In this study, an association between injury to the TCT and memory impairment after concurrent thalamic and hippocampal infarcts was elucidated using a threedimensional view of DTT.
It has been known that both the thalamus and hippocampus are involved in memory function [2,3]. Using DTT, it was demonstrated that the memory impairment in this patient was specifically caused by thalamic infarction, based on the fact that the fornix from the hippocampus was intact. However, our findings were in conflict with the results of previous reports. For example, Carlesimo et al. [3] have systematically analyzed memory function in patients with thalamic stroke using neuropsychological tests and have found that memory impairment in those patients is mainly related to the MTT. Another study has demonstrated that the integrity of the MTT was affected in patients with thalamic hemorrhage, thus leading to poor cognition [10]. However, these results are limited in how they can be applied to our patient. Previous studies exploring the relationship between memory impairment and the MTT have relied on a two-dimensional view alone without investigating other neural tracts such as the TCT, fornix, and cingulum. In addition, in the latter study, memory testing was performed with a Mini-Mental State Examination, a screening tool. On the other hand, our results correspond to the results of previous studies regarding the relationship between the neural tract and memory function evaluated with DTT. When memory impairment occurs after brain injury, damage to the TCT is the most common cause, followed by damage to the fornix and cingulum [5-9]. To elucidate the relationship between the thalamus and memory impairment, our study demonstrates that the thalamus plays a critical role in cognitive processing.
However, this study has several limitaions. First, these observations were obtained from only one case. Therefore, caution is needed when interpreting our findings, particularly in extrapolating and generalizing them. Second, the parameters of DTT were not compared to those of a normal group. Third, we were not able to examine the gray matter of the neural tracts on the two lesions, which may be a possible cause of cognitive impairment.
Nevertheless, our results suggest that the mechanism for memory impairment following cerebral infarction is related to lesions in the Papez circuit. Our findings also demonstrate that DTT might be a useful tool for clarifying injury to the neural tract in the Papez circuit.