INTRODUCTION
Ankylosing spondylitis (AS) is a chronic inflammatory disease with progressive features, the primary affecting sites of which are the joints of the pelvis and the axial skeleton [1]. It has been reported that AS affects approximately 0.1% of the population [2]. In addition, AS may affect peripheral joints, the skin, eyes, or bowel, and also increase the risk of cardiovascular or pulmonary manifestation [3]. The reduced spinal mobility that occurs in the disease is the result of the progressive ossification and fusion of the vertebral joints caused by inflammation [4].
To evaluate structural changes to the vertebrae in AS, the modified Stoke Ankylosing Spondylitis Spine Score (mSASSS) is commonly used. This assesses the anterior corners of the cervical and lumbar vertebra. Several reports have suggested that the structural damage of the spine presented in radiographic findings is associated with impaired spinal mobility [5-9]. However, controversy exists in the literature regarding the relationship between spinal radiographic findings and spinal mobility [6,8-11].
Some previous research has suggested that impairment of spinal mobility, along with chest wall immobility, may be one of the factors that cause pulmonary dysfunction in AS [4,12-14], although other researchers have reported that the primary target of pulmonary manifestation in AS may be lung parenchyma [15,16]. Pain and stiffness caused by inflammation in the spine, as well as immobility of the chest wall and the spine, may also contribute to the decline of pulmonary function in this patient group [12,13,17].
Fatigue presents as a feeling of exhaustion and a lack of energy with reduced capacity and efficiency in work [18-20]. More than 50% of patients with AS complain of fatigue [21,22], and the condition has been suggested to be linked to disease activity, functional level, pain, stiffness, mood, and occupational capability [18,22-24]. However, the clinical impact of the aforementioned factors on fatigue in this population remains unclear.
Quality of life (QOL) is an important outcome in patients with chronic disease. There have been a few reports related to QOL in patients with AS [25], with a recent report revealing an association between spinal mobility and QOL in patients with AS [26].
In light of the relative scarcity of research in this area, the aim of the current study was to assess spinal mobility, radiographic changes in the spine, pulmonary function, pain, fatigue, and QOL in patient with AS, and to reveal the relationship between these variables.
MATERIALS AND METHODS
Thirty-six adult patients with AS were recruited from the outpatient department. All participants were outpatients diagnosed using the modified New York criteria [27]. The exclusion criteria were: 1) other musculoskeletal problems in the spine or thoracic cage, 2) cardiopulmonary disease, and 3) a concurrent medical condition that could be reasonably expected to affect the patient's functional level or QOL.
The SF-36 Health Survey (SF-36) was employed to evaluate the QOL of participants. This measure consists of 36 items, and answers are scored and summed to produce a value from 0 to 100 for each of the eight domains (physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health) as well as to give an overall score [28]. The Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), the Bath Ankylosing Spondylitis Functional Index (BASFI), and the Multidimensional Assessment of Fatigue (MAF) scale were used to assess participants' disease activity, functional impairment and degree of fatigue, respectively. The BASDAI has six questions related to fatigue, back pain, peripheral pain, peripheral swelling, local tenderness, and morning stiffness (severity and duration). Other than the item relating to morning stiffness, all questions are scored from 0 (none) to 10 (very severe) using a visual analogue scale (VAS). The average of the first five questions becomes the final score, with a higher score indicating more severe disease activity [29-31]. The BASFI is comprised of ten questions assessing functional limitations and the level of physical activity at home and work. VAS is used to score each question from 0 (easy) to 10 (impossible), and the average value over the 10 questions is the BASFI score [32]. The MAF assess the degree of fatigue by employing 16 items using a Numeric Rating Scale, and scores for 15 items are transformed into a score from 0 (no fatigue) to 50 (severe fatigue) [33-35]. Participants' perceived physical condition and degree of pain (pain in any joint, back pain, and nocturnal back pain) during the last week were assessed by using a 10 cm VAS. We also collected participants' general characteristics including their sex, age, weight, height, and the date of onset and diagnosis. All questionnaires were given to participants with detailed instructions and demonstrations and were returned to us by mail.
Participants' spinal mobility was also examined through seven physical tests: 1) modified Schober test, 2) lateral bending, 3) chest expansion, 4) occiput to wall, 5) finger to ground, 6) bimalleolar distance, and 7) the range of motion (ROM) for the cervical and thoracolumbar spine, as measured by inclinometer. Vertebral squaring was also evaluated through the mSASSS of the cervical and lumbar spine. Plain radiographs of the cervical and lumbar spine were obtained, and the anterior angles of the cervical vertebra (lower C2 to upper T1) and lumbar vertebra (lower T12 to upper S1) were scored. Each anterior vertebral angle was scored at 0 (normal), 1 (erosion, squaring, or sclerosis), 2 (syndesmophyte) or 3 (bridging), with total scores ranging from 0 to 72 [36]. The mSASSS was scored by a musculoskeletal radiologist. Pulmonary Function Test (PFT) was performed using a MicroPlus Spirometer (CareFusion Corporation, San Diego, CA, USA), and the forced expiratory volume in one second (FEV1), forced vital capacity (FVC) and FEV1/FVC values were obtained. The PFT was performed three times for each participant, so that the best result could be obtained.
The Spearman coefficient was used to see the correlation among variables. A p-value of less than 0.05 was considered to be significant in all analyses. Data analyses were performed using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA) for Windows.
RESULTS
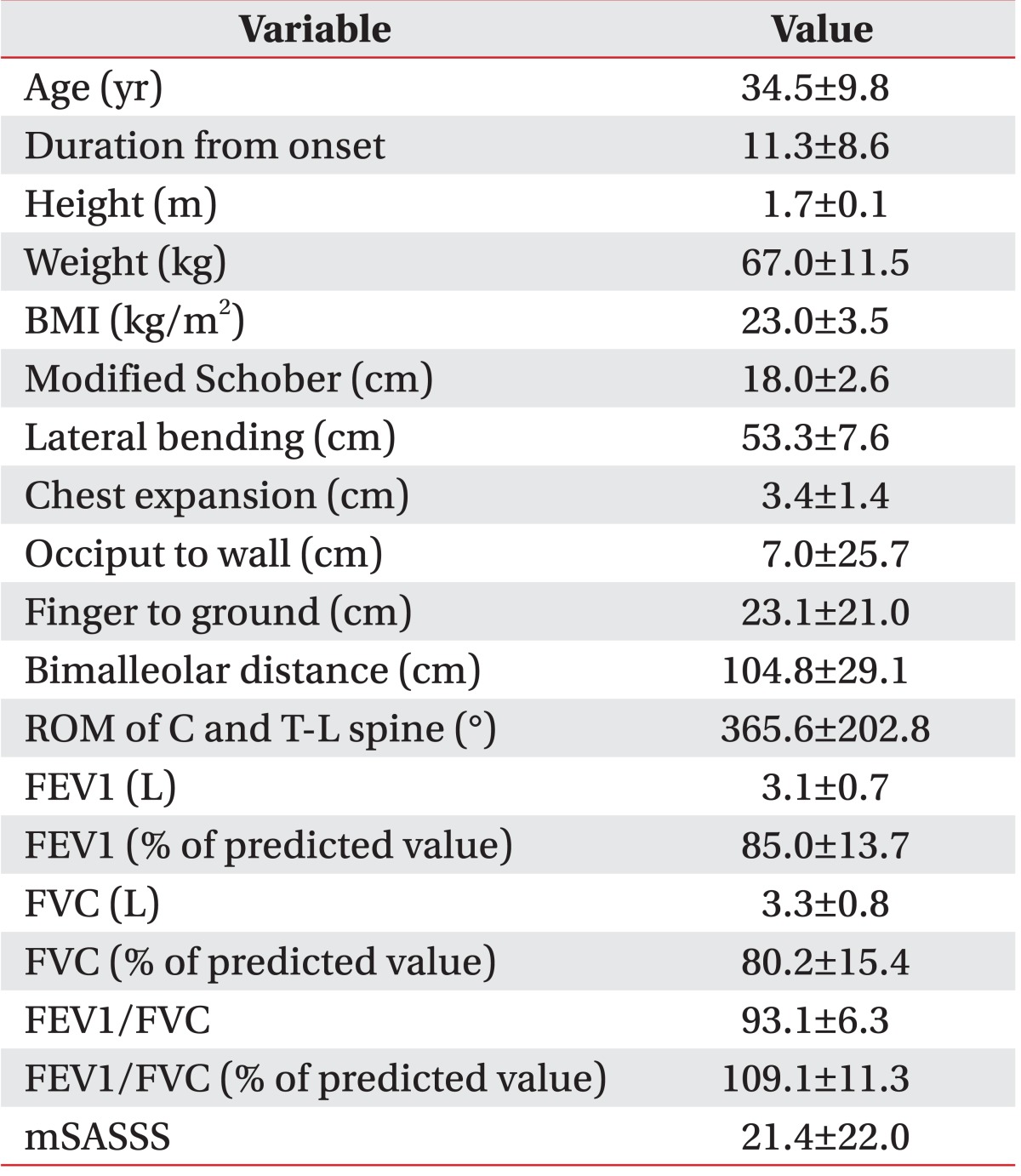
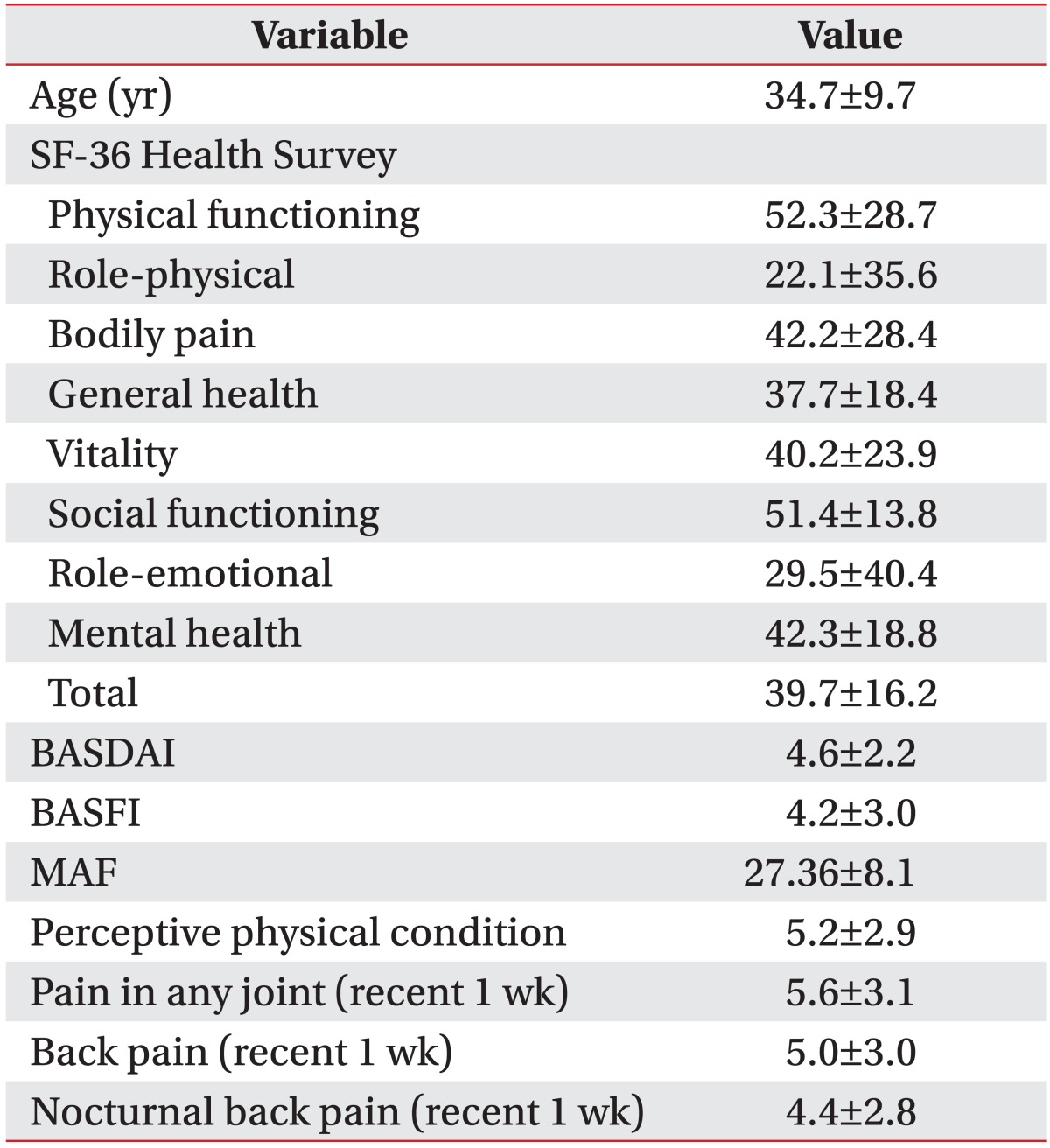
Of thirty-six participants, thirty-one were males (86.1%) and five were females (13.9%). Their mean age was 34.5±9.8 years (ranging from 24 to 52 years) and the mean duration from the onset was 11.3±8.6 years (ranging from 0.1 to 26 years). They showed reduced spinal mobility in physical examination, and their mean combined ROM of the cervical and the thoracolumbar spines was 365.6°±202.8° (Table 1). The mean mSASSS of participants was 21.4±22.0. When we analyzed their PFT results, a restrictive pattern was revealed with reduced FEV1 (85.0%±13.7% of predicted value) and FVC (80.2%±15.4% of predicted value) and increased FEV1/FVC (109.1%±11.3% of predicted value) (Table 1). Only twenty-six participants replied to the questionnaire items, including SF-36, BASDAI, BASFI, and MAF, and their mean age and duration from onset were 34.7±9.7 and 13.2±8.8 years, respectively. Their QOL, disease activity, functional level, fatigue, and pain are described in Table 2.
Relationship between spinal mobility and structural changes of the spine
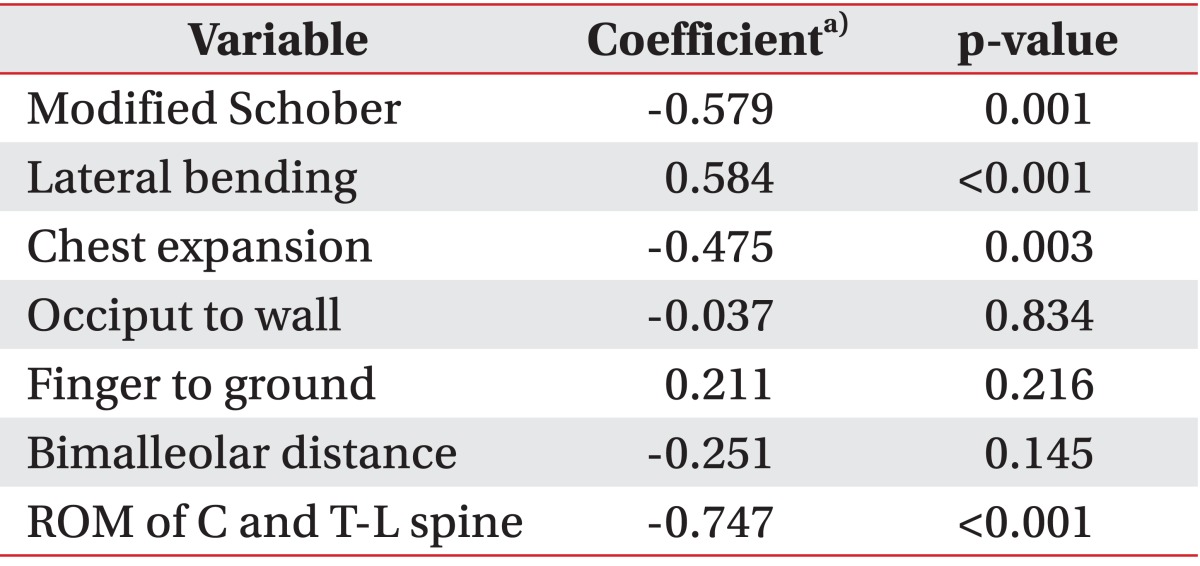
The mSASSS score was negatively correlated with modified Schober test, chest expansion, and ROM of the spine, whereas it was positively correlated with lateral bending. Other physical examination results did not show any significant correlations with mSASSS. The ROM of the spine showed its strongest relationship with mSASSS (coefficient, -0.747; p<0.001) (Table 3).
Pulmonary function: the relationships with spinal mobility and structural changes of the spine
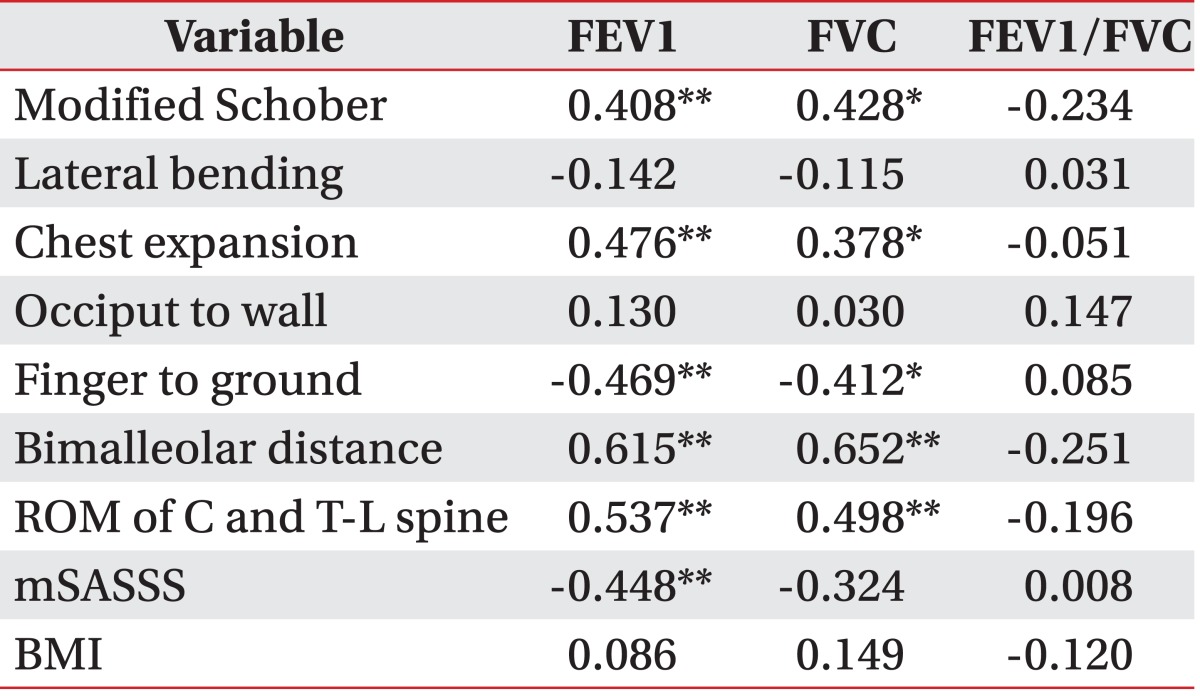
Both FEV1 and FVC showed positive correlations with modified Schober test, chest expansion, bimalleolar distance, and ROM of the spine and showed negative correlations with finger to ground. FEV1 was also negatively correlated with mSASSS (coefficient, -0.448; p<0.01). There was also a negative correlation between FVC and mSASSS, but this was not statistically correlated (coefficient, -0.324; p=0.06). However, all variables related to spinal mobility or mSASSS were not correlated with FEV1/FVC. The body mass index did not show any significant correlations with FEV1, FVC, or FEV1/FVC (Table 4).
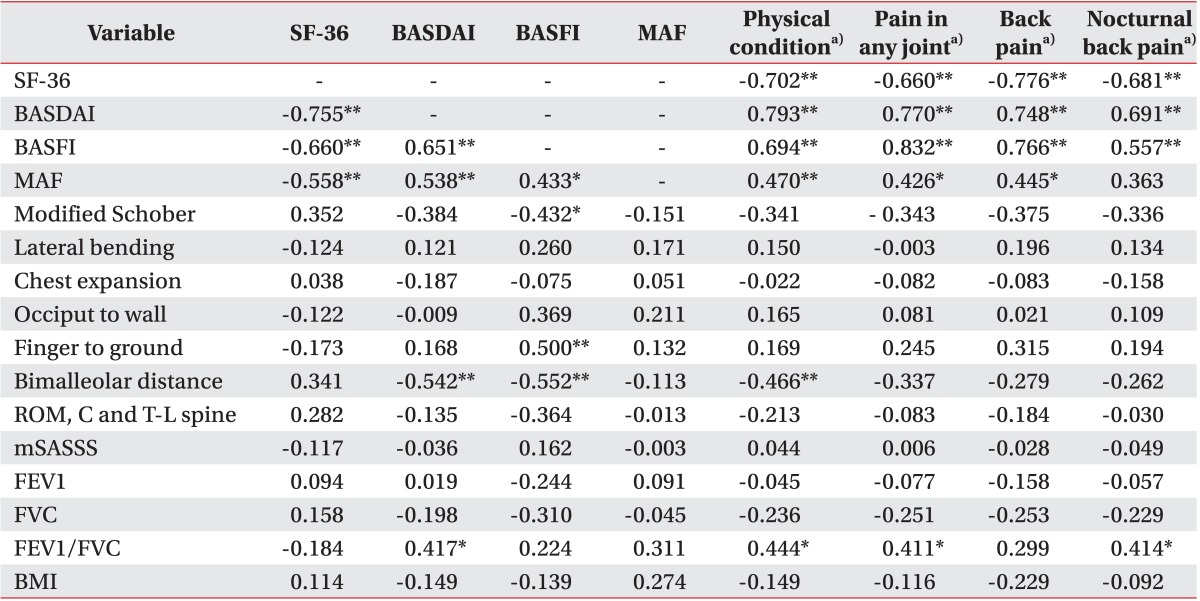
The relationships among QOL, disease activity, functional level, fatigue, and pain
MAF had a negative correlation with SF-36 and positive correlations with BASDAI and BASFI (Table 5). Perceived physical condition, pain in any joint, and back pain were all negatively correlated with SF-36, whereas they were positively correlated with BASDAI, BASFI, and MAF. Nocturnal back pain also showed a negative correlation with SF-36 and a positive correlation with BASDAI and BASFI. However, the correlations between nocturnal back pain and MAF were not statistically significant (coefficient, 0.363; p=0.068) (Table 5).
QOL, disease activity, functional level, fatigue, and pain: the relationships with other variables
BASFI was positively correlated with finger to ground and negatively correlated with modified Schober test and the bimalleolar distance. There was also a negative correlation between BASDAI and the bimalleolar distance. However SF-36, BASDAI, BASFI, and MAF did not show any consistent relationships with modified Schober test, lateral bending, chest expansion, occiput to wall, finger to ground, bimalleolar distance, or ROM of the spine (Table 5). SF-36, BASFI, and MAF were not significantly correlated with pulmonary function, and only BASDAI showed a positive correlation with FEV1/FVC (coefficient, 0.417; p=0.038) (Table 5). Perceived physical condition, pain in any joint, and nocturnal back pain were all positively correlated with FEV1/FVC, but there were no other correlations found between the patient's perceived physical condition and pain and other variables, including ROM, mSASSS, FEV1 and FVC (Table 5).
DISCUSSION
This study was conducted in patients with AS to evaluate their spinal mobility, the spinal radiographic findings, pulmonary function, QOL, pain and fatigue, and to assess the relationships among these outcomes. Previous research has shown inconsistent results for the relationship between the radiographic findings and spinal mobility [5-10]. Our results suggest that more severe radiographic changes in the spine are related with reduced spinal mobility and chest wall motion, which was confirmed in the ROM of the spine as assessed by inclinometer and the results of three physical examinations (modified Schober, lateral bending, and chest expansion tests).
The pulmonary function of patients with AS is known to show a restrictive pattern caused by stiffness and interstitial lung disease [13,15,37-39], and patients in this study also showed some restrictive patterns in PFT with increased FEV1/FVC and reduced lung capacity. Reduced FEV1 was another result indicated by our study. These findings may reinforce previous reports that there is small airway involvement in the reduced volumic airway conductance seen in patient with AS [13,15]. Both reduced FEV1 and FVC were related to reduced spinal mobility and spinal radiographic changes. This result implies that spinal mobility assessment, as well as radiographic changes in the vertebral body, may have a predictive value for the respiratory vital capacity of patients with AS, and this finding can be applied to predict pulmonary function and to provide appropriate rehabilitative interventions in clinical settings. However, FEV1/FVC showed no relationship with either spinal mobility or radiographic changes, which may be explained by the fact that both FEV1 and FVC were reduced simultaneously.
This study also shows that there are significant relationships among decreased QOL, more severe disease activity, greater impairments in functionality and a higher degree of fatigue, results which correspond with the findings of earlier study [25].
Previous research has reported that pulmonary impairments can reduce exercise capacity [40], and may also affect functional level and QOL [38]. Spinal mobility is also known to impair the QOL in patients with AS [26,37]. However, our study revealed that QOL and functional level were not related to spinal mobility, radiographic changes in the spine or PFT. This result may be related to reports that cardiopulmonary fitness is more important than is spinal mobility, chest expansion or lung capacity. Fisher et al. [4] reported that patients with AS may maintain an adequate work capacity by carrying out regular exercise with modest intensity, irrespective of spinal or chest wall immobility with reduced vital capacity. Another study has revealed that the functional capacity of patients with AS was not significantly influenced by spinal and chest wall immobility with a restrictive pulmonary pattern, as confirmed by PFT, and emphasized the role of moderate physical activity within an active lifestyle for maintaining exercise tolerance [14]. In this study, poorer perceived physical condition and more severe pain were significantly related with decreased QOL, more severe disease activity, greater impairments to functionality, and a higher degree of fatigue. This result implies that pain and perceived physical condition may both have an important role in QOL, functional capacity, and fatigue in patients with AS, although we should take into account that both the BASDAI and SF-36 include items related to pain and physical condition. That said, the results suggest that we may need to focus on pain management and encouraging AS patients to maintain good physical activity levels, in addition to improving spinal mobility or preventing structural changes of the spine.
This study has a limitation in that it was a cross-sectional study, and as such extended study in a larger population with a long-term follow-up will be required to confirm the relationship between the changes of each parameter assessed in this study. Considering additional parameters such as the maximum oxygen capacity would also be helpful in clarifying the role of cardiopulmonary fitness in this model.
In conclusion, this study shows that both spinal mobility and radiographic changes in the vertebral body may have a predictive value for pulmonary impairment in patients with AS, and can be applied to predict pulmonary function in clinical settings. We also suggest that providing appropriate pain management and recommending the maintenance of a good physical activity level may be important in improving the QOL and functional capability of patients with AS.