INTRODUCTION
Supraspinatus atrophy can occur secondary to pathologies of the central and peripheral nervous system, as well as muscular and tendinous pathology. Supraspinatus is an important target muscle for functional electrical stimulation when there is weakness of shoulder muscles in stroke patients.1 Rupture of the supraspinatus tendon causes degeneration and atrophy of muscles and this is known to influence prognosis after surgery.2 Evaluation of the extent of supraspinatus atrophy is expected to confer benefits to patients experiencing pathologies of the central and peripheral nervous system, as well as muscular and tendinous pathology.
Although the standardized imaging method for assessing supraspinatus atrophy has been magnetic resonance imaging (MRI),3 advances in ultrasonographic imaging technology have lead to high correlation with MRI in assessing supraspinatus atrophy.4 The portion of supraspinatus sectional area in the supraspinatus fossa demonstrated by the Y-view of MRI is suitable for the measurement of atrophy,5 and it has also been possible to demonstrate this by using ultrasonography.4
However, subjective factors are known to influence ultrasonographic examinations which do not influence MRI, and evaluation with ultrasonography concurrently leads to divergent results. Moreover, ultrasonography cannot penetrate the skeleton. The Y-view of MRI can visualize the most bony surrounded section at the shoulder such as clavicle anteriorly, supraspinatus fossa inferiorly, scapular spine posteriorly, trapezius muscle superiorly.5 It is therefore possible for the Y-view not to be examined using ultrasonography.
The purpose of this study was to evaluate the test-retest reliability for eliminating subjective factors and reliability of a follow-up study in ultrasonographic examination, and to verify the relationship between the tracing and ellipsoidal methods. In addition, this study investigated the practical availability of assessing the occupational ratio of supraspinatus fossa in Y-view using ultrasonography.
MATERIALS AND METHODS
Subjects
Twenty two supraspinatus muscles in 11 normal individuals were assessed in this study. Every subject was male with an average age of 26.5 years (standard deviation (SD)=3.5 years). There was no history of shoulder pain and sonographic abnormality in the supraspinatus muscles of the subjects.
Methods
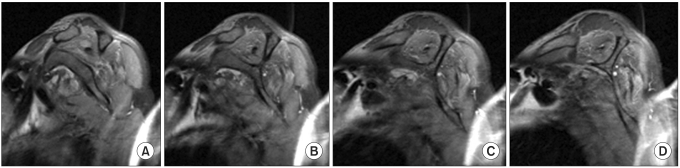
To scale the size of the supraspinatus, we applied the occupational ratio in the supraspinatus fossa proposed by Thomazeau et al.5 The occupational ratio on the MRI Y-view was established by measuring the portion of the supraspinatus in the supraspinatus fossa. The Y-view is a sagittal oblique view of the shoulder joint, which passes through the medial side of the coracoid process, and is surrounded by a bony area (Fig. 1).
Ultrasonographic examination was performed by a physiatrist with over 6 years of clinical experience. A linear probe of 5-12 MHz was used (HD11XE, Philips Medical Systems, Bothell, USA). To standardize the evaluation, all subjects sat in a chair with their arm laid on the side of the body, while the shoulders were in neutral position and the elbows were fully extended.
The modified Khoury's method was used for sonographic reproduction of the MRI Y-view to obtain occupational ratio.4 First, we identified the scapular notch in the coronal view, and then the probe was perpendicularly rotated to obtain a sagittal oblique view. By moving the probe from medial to lateral, we obtained a view in which the entire supraspinatus muscle was visualized, and calculated the occupational ratio by dividing the area of the supraspinatus muscle by the supraspinatus fossa area.
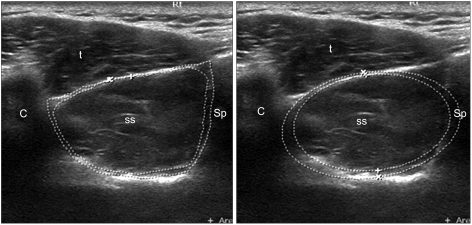
Two methods were used to obtain the cross-sectional area. First, the tracing method was applied, which tracked lines with boundary. Second, was the ellipse tool method, which established an ellipse as a boundary. For the tracing method, the cross sectional area of the supraspinatus muscle was measured at the closest boundary of the muscle. The borders that defined the portion of supraspinatus fossa was set by the internal bony boundary of the Y view, consisting of the clavicle anteriorly, the cortex of the supraspinatus fossa inferiorly, the scapular spine posteriorly and the inferior border of the trapezius superiorly. For the ellipse tool method, the ellipse was set at the closest line that included the supraspinatus muscle. The border of the supraspinatus fossa was defined by the closest line, including the supraspinatus fossa through the internal bony boundary of the Y-view (Fig. 2).
Two measurements were performed within 7 days to evaluate test-retest reliability. By using the SPSS 14.0 software (SPSS Inc., Chicago, USA), the test-retest reliability was evaluated by calculating the Pearson correlation coefficient and intraclass correlation coefficient (ICC).
RESULTS
The occupational ratios of the 11 normal subjects were 0.71-0.96 (mean value of 0.86) by the tracing method, and 0.69-0.96 (mean value of 0.85) by the ellipsoidal method. The Pearson correlation coefficient of the two method was 0.80 (p<0.05).
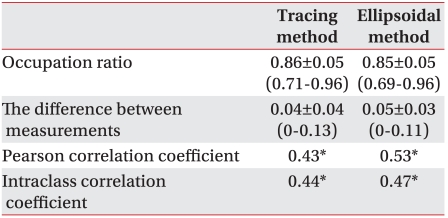
The difference between the two measurements in the evaluation of test-retest reliability was 0-0.13 (mean value of 0.04) for the tracing method, and 0-0.11 (mean value of 0.05) for the ellipsoidal method. The Pearson correlation coefficient was 0.43 for the tracing method and 0.53 for the ellipsoidal method. ICC of two measurements was 0.44 for the tracing method and 0.47 for the ellipsoidal method (Table 1).
DISCUSSION
In this study we measured both shoulders of 11 normal subjects (22 shoulders). The occupational ratio of supraspinatus muscle was over 0.71 for the tracing method and over 0.69 for the ellipsoidal method, which is within the normal limits according to Thomazeau's classification. Thomazeau et al.5 measured the occupational ratio of the supraspinatus muscle in the supraspinatus fossa and defined a range between 0.60 and 1.00 as being representative of normal or mild atrophy, 0.40 and 0.60 as being representative of moderate atrophy and less than 0.40 as being severe atrophy.
Because both the tracing and ellipsoidal methods were highly correlated (r=0.80), it is suggestive that the ellipsoidal method can be used clinically as much as the tracing method. However, the tracing method remains a standard that demonstrates the severity of supraspinatus atrophy more clearly. Further studies are needed for determining the significance of measuring cross-sectional areas of the supraspinatus muscle in patients with stroke, rotator-cuff tear and shoulder pain.
The test-retest reliability of ultrasonography was relatively low.6 A major reason may be narrow range of measurement. Mean values of the two methods were 0.85 (SD=0.05) for the tracing method and 0.85 (SD=0.05) for the ellipsoidal method. If the values were distributed from low to high range, the correlation coefficient would be high. However, this study assessed only normal adult males, therefore the measured values were distributed within a similar range, and this resulted in a relatively low correlation coefficient. The maximal difference between the ratios was not high. The mean difference was 0.04 in the tracing method and 0.05 in the ellipsoidal method. The maximum difference was 0.13. Although the test-retest reliability was low, further studies including stroke patients and those with supraspinatus muscle lesions are required.
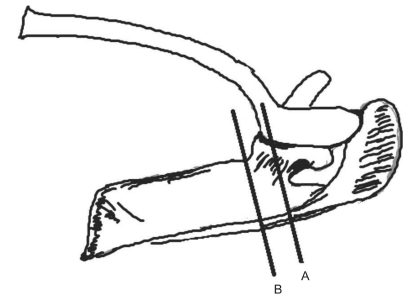
T1 enhancing image in MRI is the standard method to estimate supraspinatus muscle atrophy, and the sectional area of supraspinatus muscle can be obtained from the Y-view passing through the medial border of the coracoids process for the sagittal oblique view of the supraspinatus fossa.5 Currently, advances in ultrasonographic technology have lead to an increase in its application in musculoskeletal disorders, and the MRI Y-view can be reproduced by ultrasonography.4 However, because the Y-view is the most bony section surrounding the supraspinatus fossa, it remains challenging to obtain it using ultrasonography (Fig. 3). In this study, the sectional area of supraspinatus muscle was frequently not obtained at the section of Y-view because of the clavicle.
To obtain the Y-view using ultrasonography, the probe must be located longitudinal to the supraspinatus muscle, and then tilted to the deep side of the scapular spine to seek the scapular notch. After seeking the scapular notch, the probe would need to be rotated perpendicularly from the direction of the supraspinatus muscle. If the examiner can visualize the section of the supraspinatus muscle around this point, this can be considered as the Y-view (Fig. 3). If the examiner cannot visualize the entire supraspinatus muscle, the probe will need to be moved medially or laterally to obtain the entire supraspinatus muscle. Echogenecity of the bone must be observed anteriorly, inferiorly and posteriorly. The examiner should observe the clavicle anteriorly, the suprascapular fossa inferiorly and scapular spine posteriorly. Only one or two Y-views can be obtained on MRI because excessive lateral view contains the spinoglenoid notch and excessive medial view contains the scapular notch anteriorly. However, because the clavicle may overlap the supraspinatus muscle anterosuperiorly at this point, the probe may be moved a small amount medially (Fig. 3). In other words, Thomazeau's method could not trace the supraspinatus muscle because of the overlap of the supraspinatus muscle and the clavicle anterosuperiorly. That may be the reason why Thomazeau used the ellipse tool method in place of the tracing method. However, if the examiner moves the probe medially to avoid overlapping the clavicle and to locate the most lateral side of the whole section of supraspinatus, it is possible to trace the section of supraspinatus muscle. The most accurate way to measure the muscle's atrophy is by measuring the volume of the muscle. Continuative cross sectioning of the bone can mathematically calculate the volume.7,8 Nevertheless, some reports suggest only one cross sectional area for the measurement of atrophy. This method also appears to have clinical usefulness. There are reports that suggest measuring the width of the muscle correlates with the cross sectional area.9 Ultrasonography measures the cross sectional area accurately. As it is simpler to measure the thickest part of the cross section, it will be interesting to further investigate the clinical usefulness of measuring muscle thickness.
The limitations of this study are as follows. First, reliability between examiners was not measured. Second, women and elderly subjects were not evaluated in this study. In women or elderly subjects, muscular atrophy is common, and degenerated muscle is indistinguishable from fat tissue. Therefore, it remains challenging to confirm the border of the muscle in these populations. In addition, it can worsen following muscle atrophy in patients with pathologic shoulders, including shoulder pain and stroke.
CONCLUSION
In this study, the occupational ratio of the supraspinatus muscle was evaluated using ultrasonography in twenty two shoulders of eleven normal male adults. This method had low test-retest reliability, but maximum deviation was not high. Thus further studies are needed targeting patients with supraspinatus muscle atrophy due to rotator-cuff tear or stroke.