INTRODUCTION
Hand strength has been widely used in clinical practice as an objective index for functionality of the upper limbs.1,2 It is very important to measure hand strength accurately because it can serve as an indicator of the progress of treatment and rehabilitation of the damaged hand.3 The importance of measuring hand strength has been emphasized in the past: in 1985, Mathiowetz et al.4 stated that normative data of hand strength are required for the assessment of patients, to set a practical treatment goal and to make a vocational evaluation in order for patients to return to work.
Hand strength can be obtained by measuring several kinds of pinch strength such as grip strength, tip strength, key pinch strength and tripod pinch strength.3 The Jamar grip dynamometer and Jamar pinch gauge are the most widely used instruments for measuring grip and pinch strength.5,6 Since first introduced by Bechtol7 in 1954, the Jamar grip dynamometer has shown high inter-instrumental and inter-rater reliability in many studies.8 Also, it has standard values for adults and children which can easily be used clinically.9 However, the Jamar grip dynamometer requires frequent calibration to maintain its reliability, and reading with an analogue scale may result in measurement error.10
During the past 20 years, a number of digitalized dynamometers have been used in clinical practice. But the existing normative values for grip strength were taken by the Jamar grip dynamometer, so they have many restrictions in comparison with the values from digitalized measuring instruments. To this end, studies on the reliability between the digital dynamometers, like DynEx11 and Computerized Jamar Dynamometer,12 and between these instruments and the Jamar grip dynamometer, which is the standard instrument, have been carried out.
In contrast to the international case, the domestic development of digitalized measuring instruments is a relatively new phenomenon resulting in the analogue Jamar dynamometer still being used clinically in South Korea. The purpose of this study is to verify whether the Digitalized Pinch Dynamometer (Fig. 1) developed at our institute can be used clinically; this was done by conducting tests of inter-test and inter-rater reliability in measuring key pinch, and by comparing the results of this dynamometer with those of the hydraulic Preston pinch gauge (Sammons Preston, Illinois, USA), which is now being used in our Occupational Therapy Center.
MATERIALS AND METHODS
Subjects
Subjects consisted of 30 healthy adults (23 males, 7 females) aged 23-33 years. They had an average age of 27.8 years (male: 28.1, female: 27.7), average height of 173.5 cm (male: 176.4±5.7, female: 168.8±7.4) and average weight of 68.6 kg (male: 74.3±7.3, female: 61.2±13.7). 23 of the subjects were right-handed (76.7%) and 7 were left-handed (23.3%).
All subjects had no lesion or history of lesion of the nervous, muscular and skeletal system which might affect their hand functionality. Those who had injury or pain at the time of the test were excluded (Table 1).
Digitalized Pinch Dynamometer
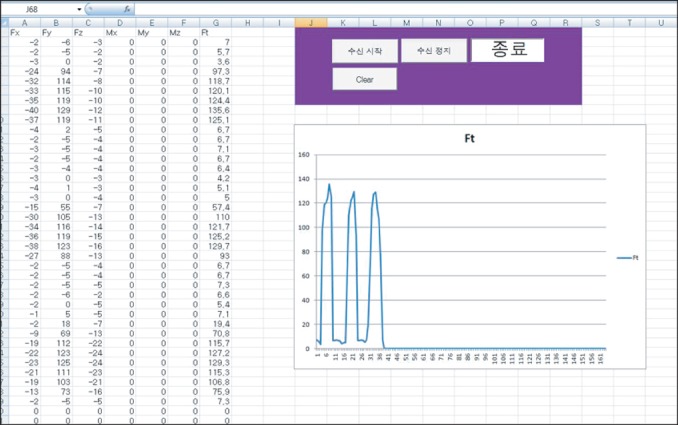
The Digitalized Pinch Dynamometer is a measuring instrument designed and developed by our Control and Measurement Engineering Department. It consists of a high-speed gauge and a two-fingered power measurement device. The two-fingered power measurement device uses the 3-axis power sensor method that allows precise measurement at 10-gram intervals. It measures the pressing power of two fingers and sends the measured values to a high-speed gauge to calculate the force, which Fig. 1. Digitalized Pinch Dynamometer. is displayed on the LCD and transmitted to the computer simultaneously. The measured values are transmitted to the computer every 0.8 second and these measurements are converted into a force graph which is displayed on the computer screen (Fig. 2).13
Methods
We used the Preston Pinch Gauge (Fig. 3) and Digitalized Pinch Dynamometer to measure pinch strength. Measurement was achieved by pressing the front part of the thumb together with the side part of the index finger (Fig. 4) in the standard position proposed by the American Society of Hand Therapists.14,15 In this position, subjects were seated in a chair, with their shoulders adducted and neutrally rotated, their elbows flexed 90 degrees, their forearms positioned neutrally, and their wrists flexed in 0-30 degrees and 0-15 degrees of ulnar deviation (Fig. 5). At first, rater 1 informed the subjects about the measurement procedure and gave them a verbal command to exert their maximum strength for 3 to 5 seconds. Mean values were recorded after measuring three consecutive tests with both their hands. According to those procedures, pinch strengths of the subjects' left and right hand were measured with the Preston Pinch Gauge, and then with the Digitalized Pinch Dynamometer after a 10-minute break. After this, pinch strength was measured again with the Digitalized Pinch Dynamometer after 10 minutes in order to evaluate the inter-instrumental reliability of the dynamometer. Rater 2 conducted the measurement in the same way one hour after the testing by rater 1 was concluded. The results of measurement of the two raters were kept hidden from the other rater.
Statistics
We used statistical analysis tool SPSS version 17.0, and performed a paired T-test to check the difference of the measured values between the Preston Pinch Gauge and Digitalized Pinch Dynamometer. Intraclass correlation coefficient (ICC) was used to evaluate inter-instrumental and intra-rater reliability of the measurement. In this study, it was considered statistically significant when the p-value was 0.05 or less.
RESULTS
Pinch strength measured with Preston Pinch Gauge and Digitalized Pinch Dynamometer
The mean values of measurement with the Preston Pinch Gauge were: 9.65±1.21 kg (right), 8.87±1.51 kg (left) for males, and 6.22±1.03 kg (right), 5.98±1.62 kg (left) for females (Table 2). The mean values of measurement with Digitalized Pinch Dynamometer conducted by rater 1 were: on the first test, 9.58±1.12 kg (right), 8.91±1.53 kg (left) for males, and 6.17±0.94 kg (right), 6.17±1.64 kg (left) for females; and on the second test, 9.50±1.26 kg (right), 8.69±1.56 kg (left) for males, and 6.48±1.05 kg (right), 5.92±1.41 kg (left) for females. The mean values of measurement conducted by rater 2 were: on the first test, 9.22±1.68 kg (right), 8.31±1.67 kg (left) for males, and 6.18±1.11 kg (right), 5.80±1.26 kg (left) for females; and on the second test; 9.07±1.62 kg (right), 8.48±1.79 kg (left) for males, and 5.90±1.33 kg (right), 5.44±1.15 kg (left) for females (Table 3).
The difference between the mean values of pinch strength measured with the Preston Pinch Gauge and Digitalized Pinch Dynamometer was not statistically significant when measured by rater 1, but was significant when measured by rater 2 (Table 4).
Inter-instrumental reliability of Preston Pinch Gauge and Digitalized Pinch Dynamometer
Correlation coefficients between the pinch strength values measured with the Preston Pinch Gauge and the values measured by each rater with the Digitalized Pinch Dynamometer were 0.82 for rater 1, and 0.78 for rater 2. All the correlation coefficients were statistically significant (Table 5) (p<0.001).
Comparison between the first and the second test of Digitalized Pinch Dynamometer
Correlation coefficients between the pinch strength values measured from the first test and the second test were 0.87 when done by rater 1, and 0.88 by rater 2. All the correlation coefficients were statistically significant (Table 6) (p<0.001).
Comparison between rater 1 and rater 2 of Digitalized Pinch Dynamometer
The correlation coefficient between the pinch strength values measured by rater 1 and rater 2 was 0.75. This value was statistically significant (Table 7) (p<0.001).
DISCUSSION
The development of digitalized dynamometers began about 20 years ago. In contrast to existing analogue gauges, digitalized dynamometers have the merits of improved inter-instrumental reliability due to the digital display, accurate and precise measurement, and convenient use owing to the electronic saving and retrieval of information. However, studies on the reliability and accuracy of many of these digitalized dynamometers have rarely been done.16 Fess14 stressed the importance of examining reliability for a new assessment instrument before using it in the clinical setting.
Reliability can be described as a correlation coefficient (Pearson's correlation coefficient and ICC) and standard error.11,14,15 The ICC value of 0.75 to 0.90 can be considered as having relatively high correlation. Therefore, the results of this study show that the Digitalized Pinch Dynamometer has good intra-rater and inter-rater reliability, and also has good reliability compared with the existing Preston Pinch Gauge. So it can be concluded that the Digitalized Pinch Dynamometer is a suitable instrument for measuring pinch muscle strength.
This study adopted the standard procedures of producing high reliability found during the course of many research studies4,6,8,9,11,12,15 on accurate measurement. There was a break of 10 minutes between the end of testing with one instrument and the start of testing with the next instrument in order to reduce errors due to muscle fatigue. The measurement procedure was designed on the basis of the following studies: Mathiowetz15 set a break of 5 minutes to reduce participants' muscle fatigue in his study that compared the Rolyan dynamometer and Jamar dynamometer, Shechtman et al.11 set 10 minutes as a break time to compare the DynEx Dynamometer and Jamar dynamometer.
When it comes to comparing the mean values of pinch strength measured with the Preston Pinch Gauge and Digitalized Pinch Dynamometer, the result of the T-test showed that the measurements done by rater 1 were no different between the two instruments, but for rater 2, the measurements using the Digitalized Pinch Dynamometer were significantly lower (average 0.4 kg, p<0.05) than those using the Preston Pinch Gauge. The reason for this seems to be the normal error of individuals reported by Hinson et al.16 Another reason might be that the subjects were affected by muscle fatigue because all the tests of rater 2 were performed at the end of each test.
Niebuhr et al.12 examined grip strength of 33 normal people with the PC5030PT Computerized Jamar Dynamometer, measuring the slope of rise in the force, the peak force and the mean sustained force. In that study, it was suggested that in addition to the peak force, which is commonly used in the clinical setting, the slope of the rise in force and the mean sustained force are also clinically useful. Likewise, the Digitalized Pinch Dynamometer developed by our institute can measure real-time pinch strength, and from these values, a graph of changes in force can be obtained.
In addition to the advantages of existing digitalized dynamometers, which include digital display, accurate and precise measurement, and ability to store information, the Digitalized Pinch Dynamometer can also determine the level of participation of the subjects at the time of the test through a graph of changes in force that is created during the measurement of pinch strength. In addition, as the recent study of Weinstock-Zlotnick et al.17 shows, the visual feedback to the subjects in the form of a graph displaying changes in force on the computer screen can increase their pinch strength. Therefore, the Digitalized Pinch Dynamometer can also be used as a visual feedback training tool for hand rehabilitation of stroke patients or patients with peripheral nerve injury.
CONCLUSION
The Digitalized Pinch Dynamometer showed high inter-rater and intra-rater reliability when measuring pinch strength, and higher inter-instrumental reliability compared to existing analogue instruments. The main advantage of the Digitalized Pinch Dynamometer lies in its digitalized nature-increased accuracy due to the digital display, ease of data processing, and precise measurement. Moreover, we can also use it to check the level of participation of the subjects and as a training tool using visual feedback of pinch strength.
Therefore, we conclude that the Digitalized Pinch Dynamometer is a useful clinical instrument for measuring pinch strength.