INTRODUCTION
The literature consistently highlights a significant rise in smartphone users globally, coinciding with an increase in musculoskeletal issues related to prolonged smartphone use. Studies connect excessive smartphone use to musculoskeletal disorders like neck pain, upper extremity discomfort, and ergonomic problems due to poor posture and repetitive motions [1]. These issues impact physical health and quality of life. The widespread use of smartphones has revolutionized communication and information access, yet prolonged and frequent utilization of these devices has unveiled potential health implications. Long-term engagement with smartphones often leads to the adoption of a forward neck posture, commonly termed “text neck.” This posture, characterized by a forward head position while looking down at the screen, significantly alters the cervical spine’s natural curvature [2]. The persistent adoption of such a posture strains the muscles, tendons, and ligaments supporting the cervical spine [3]. Research indicates that the continuous application of this forward head position, typical during smartphone use, places immense stress on the cervical spine, potentially leading to musculoskeletal discomfort and an increased risk of developing chronic issues [4]. Over time, this maladaptive posture can result in structural changes, impacting the integrity of the cervical spine and potentially leading to long-term musculoskeletal issues.
Forward head posture (FHP) is characterized by the positioning of the head in front of a vertical line passing through the body’s center of gravity (COG). Studies by Hansraj [5] underscore the significant impact of neck flexion on head weight. Their research findings reveal a compelling relationship between neck flexion and increased head weight. In their investigations, it was observed that as the neck flexes forward, the effective weight experienced by the cervical spine substantially escalates. Specifically, at a 60-degree head flexion angle, the effective weight borne by the cervical spine was estimated to reach approximately 28 kg [5]. This increased head weight, caused by greater neck flexion, imposes considerable stress on the cervical spine and surrounding structures, potentially contributing to the development of musculoskeletal issues associated with prolonged FHP [6].
Prolonged pressure on neck joints due to extended FHP can disrupt signals to the brain, impacting balance and neck proprioception [7]. This sustained compression and misalignment of cervical vertebrae may interfere with neural signal transmission [8]. Such disruption could compromise the brain’s interpretation of head position and movement [9]. Balance and head-eye movement control rely on integrated input from vision, vestibular, and proprioception systems [9]. Disruptions from sustained neck joint pressure may compromise proprioception, affecting accurate spatial perception and potentially influencing coordination and balance [10]. Cervical proprioception plays a pivotal role in ensuring precise head orientation in space, maintaining trunk orientation, and contributing to overall body balance [11]. Research underscores the critical nature of cervical proprioception alongside vestibular and visual inputs for accurate orientation and effective postural control [12]. Previous studies emphasize the interdependence of these sensory systems in coordinating body movements and adjusting posture to external stimuli [13]. Moreover, a noteworthy association exists between neck pain and compromised balance as well as impaired coordination of head movements. Individuals experiencing neck discomfort often exhibit increased postural sway and encounter challenges in positioning their heads accurately [14]. This linkage between neck pain and diminished balance and head movement coordination highlights the intricate relationship between cervical proprioception, postural control, and overall musculoskeletal well-being [15].
FHP is widely recognized as a prevalent postural deviation associated with various musculoskeletal imbalances and balance disorders [16]. The maintenance of balance is a complex process involving the precise coordination of sensory inputs, including vestibular, visual, and somatosensory cues, alongside the musculoskeletal system. This intricate integration facilitates the stabilization of the body’s center of mass within its base of support, minimizing postural sway, and is integral for executing daily activities [17]. Any postural changes leading to an altered COG within the base of support may contribute to the onset of balance disorders. Notably, proprioceptive impairment linked to FHP could potentially exacerbate these issues, as compromised cervical proprioception might disrupt the accurate perception of head position and movements, thereby impacting the body’s ability to maintain a stable posture and affecting overall balance [7,18].
The Nintendo Wii Balance Board (NWBB) emerges as a cost-effective alternative to conventional force platforms for assessing balance across various conditions. Notably, the NWBB serves as a versatile tool capable of evaluating both static and quasi-dynamic balance. Previous research has established associations between FHP and alterations in postural balance, highlighting potential balance disorders arising from FHP [18]. However, an unexplored area lies in investigating the specific impact of FHP on balance utilizing the NWBB. This study aims to investigate the impact of FHP on postural stability during smartphone usage. It seeks to understand how FHP, characterized by the head’s forward positioning relative to the body’s COG, affects balance and stability or body center of pressure (COP) sway. Additionally, the research explores how smartphone use posture contributes to or worsens FHP, subsequently influencing postural control.
METHODS
Study design
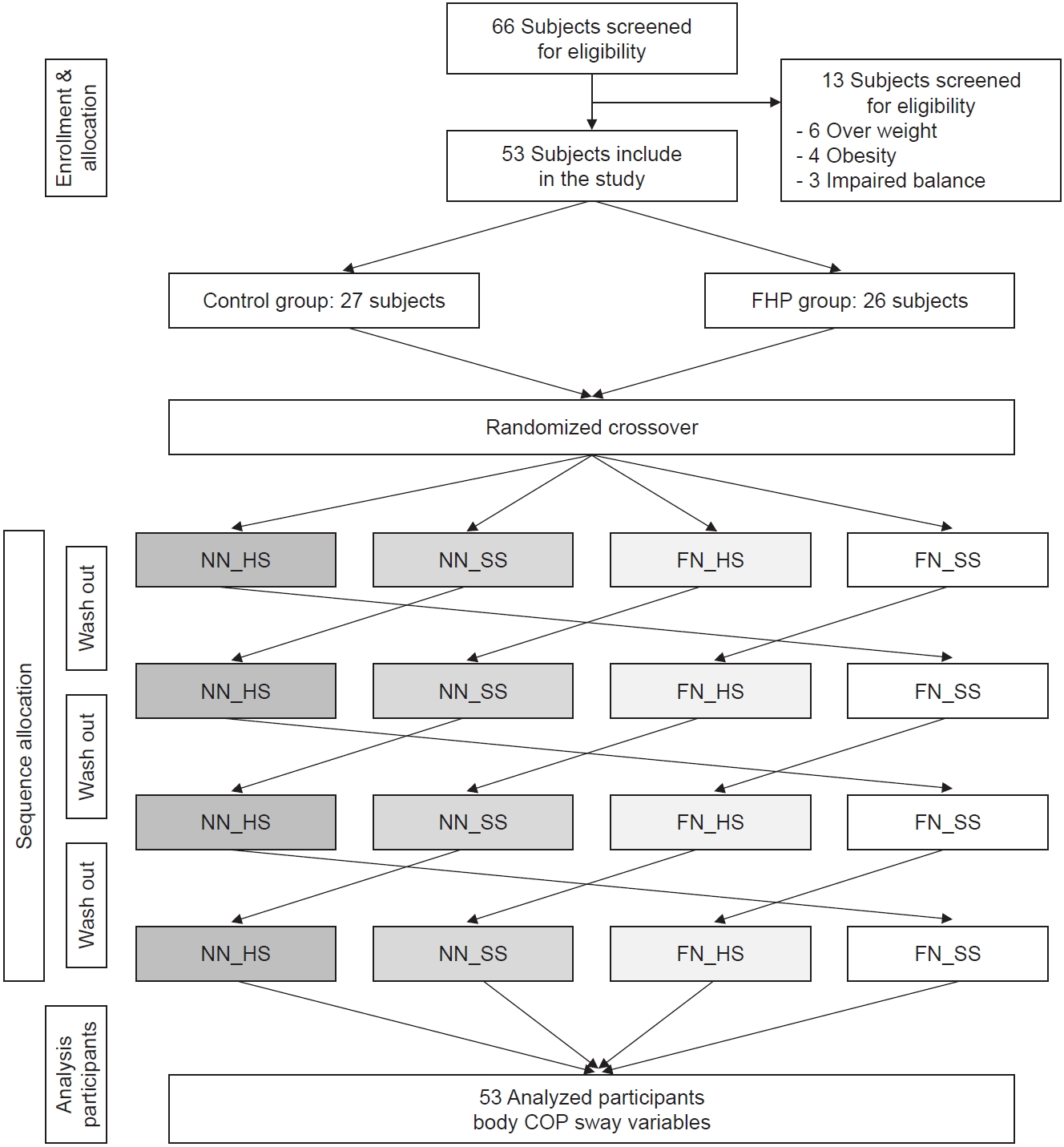
The current cross-sectional investigation utilized convenience sampling methods to recruit participants, employing printed advertisements and social media channels for recruitment purposes. This study employed a randomized repeated design, examining smartphone use in two different neck postures (neutral and flexed) across two surface conditions (hard and soft), as depicted in Fig. 1. The research took place at the Physical Therapy Laboratory, School of Allied Health Sciences, University of Phayao, Thailand. Body COP sway was evaluated using the NWBB and recorded for each condition while participants performed text typing on a smartphone and underwent a single-leg standing test on both hard and soft surfaces.
Participants
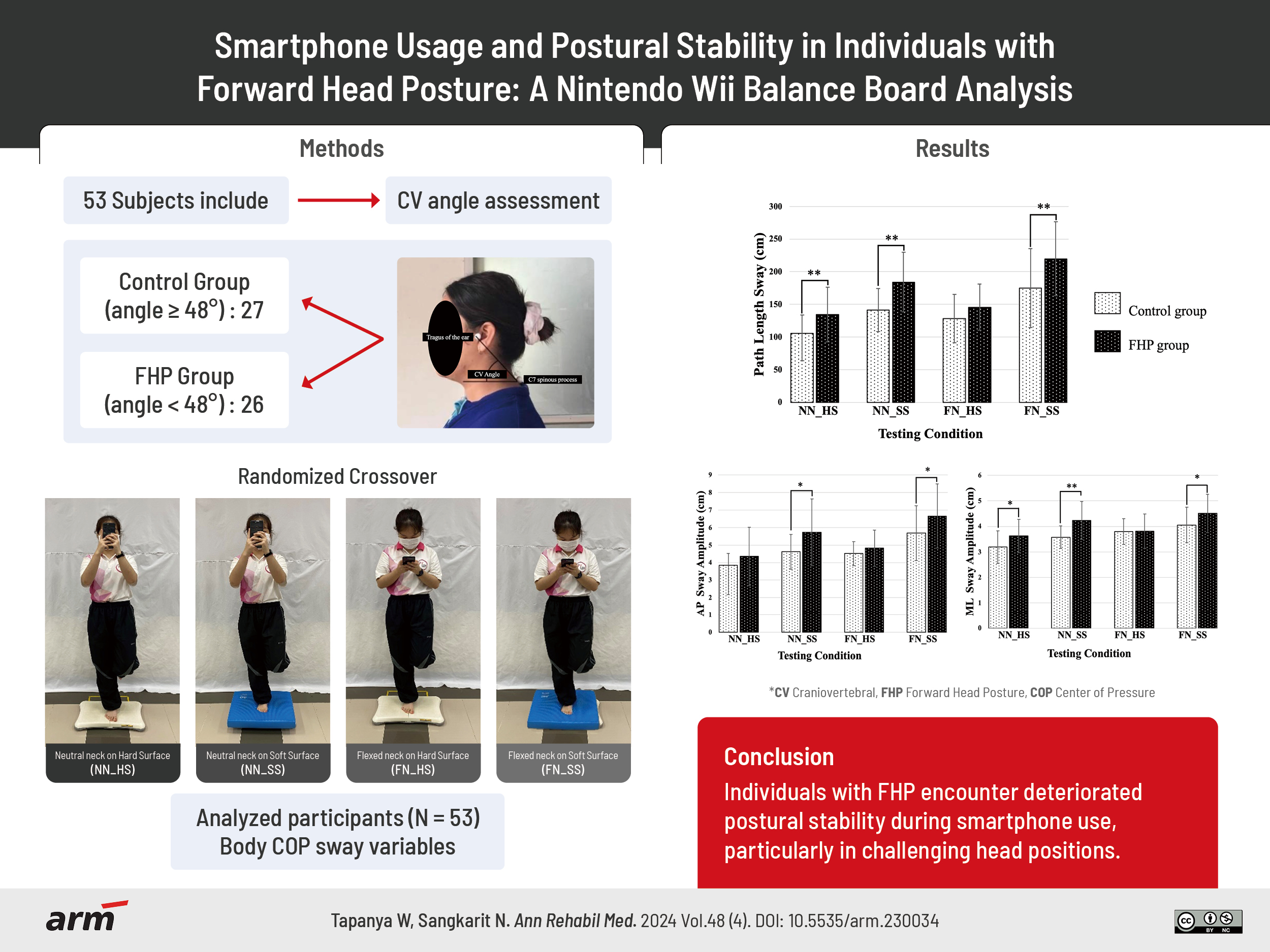
A total of 66 healthy young adults were initially enrolled in this study. However, 13 subjects were excluded due to the following reasons: 6 were classified as overweight, 4 were obese, and 3 did not pass the screening balance test. As a result, the final cohort comprised 53 subjects with equal representation of sexes and ages ranging from 18 to 25 years. Following measurement of their craniovertebral (CV) angle, subjects were categorized into two groups: a control group (n=27) consisting of those with an angle ≥48° and an FHP group (n=26) comprising those with an angle <48° [19]. All participants included in the study were exclusively right-handed and had a minimum of one year of prior experience using smartphones, dedicating an average of at least four hours daily to their device usage. Crucially, none of these participants disclosed any recent history of trauma or musculoskeletal discomfort in the neck or upper extremities within the past week. The calculation for the sample size was executed using the G*Power software, utilizing mean and standard deviation (SD) values derived from a previous study on postural sway [20]. A power calculation was conducted, with a critical α-value set at 0.05 and aiming for a robust power level of 90%. Furthermore, all participants underwent verification to confirm the absence of any neurological or musculoskeletal conditions, and they disclosed no engagement in any balance-specific training over the preceding six months. Additionally, assessing limb dominance revealed that, as per their preferred leg for kicking a ball [21], all participants displayed right leg dominance, aligning consistently with their dominant hand (i.e., their writing hand).
CV angle
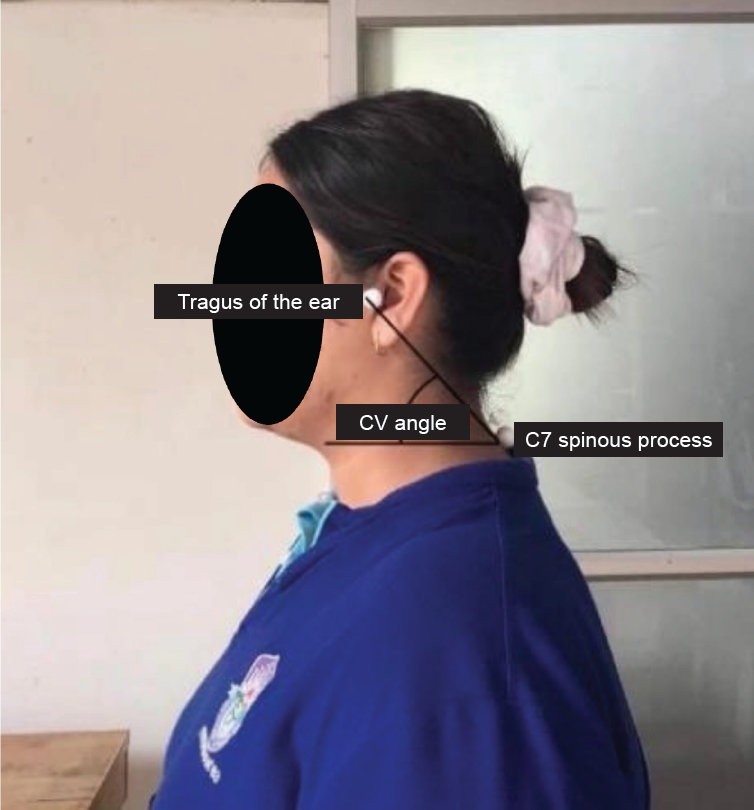
The CV angle is described as the angle formed between a horizontal line passing through C7 and a line extending from the tragus of the ear to C7. To measure this angle, photometry is utilized, employing a camera positioned at a fixed distance of 1.5 meters. The camera’s height is adjusted to match the subject’s shoulder height [22]. For accurate measurement, two markers are positioned one at C7 and the other at the ear tragus. Subjects are instructed to maintain a relaxed posture and gaze straight ahead [23]. The participant was directed to stand facing straight and was positioned laterally in front of the camera. A lateral view photograph was captured of each participant in their standing position. Subsequently, the photographs were transferred to a computer and analyzed utilizing Kinovea software. In the analysis, a virtual line was drawn between the midpoint of the tragus and the spinous process of the C7 vertebra. Additionally, a horizontal line was drawn through the spinous process of the C7 vertebra (Fig. 2). Participants exhibiting a CV angle measuring less than 48 degrees were classified as having a FHP. The reliability of CV angle measurements demonstrates strong consistency, with a test-retest reliability ranging between 0.85–0.86 and an inter-examiner intraclass correlation coefficient (ICC) of 0.88–0.89 [24].
Experimental protocol
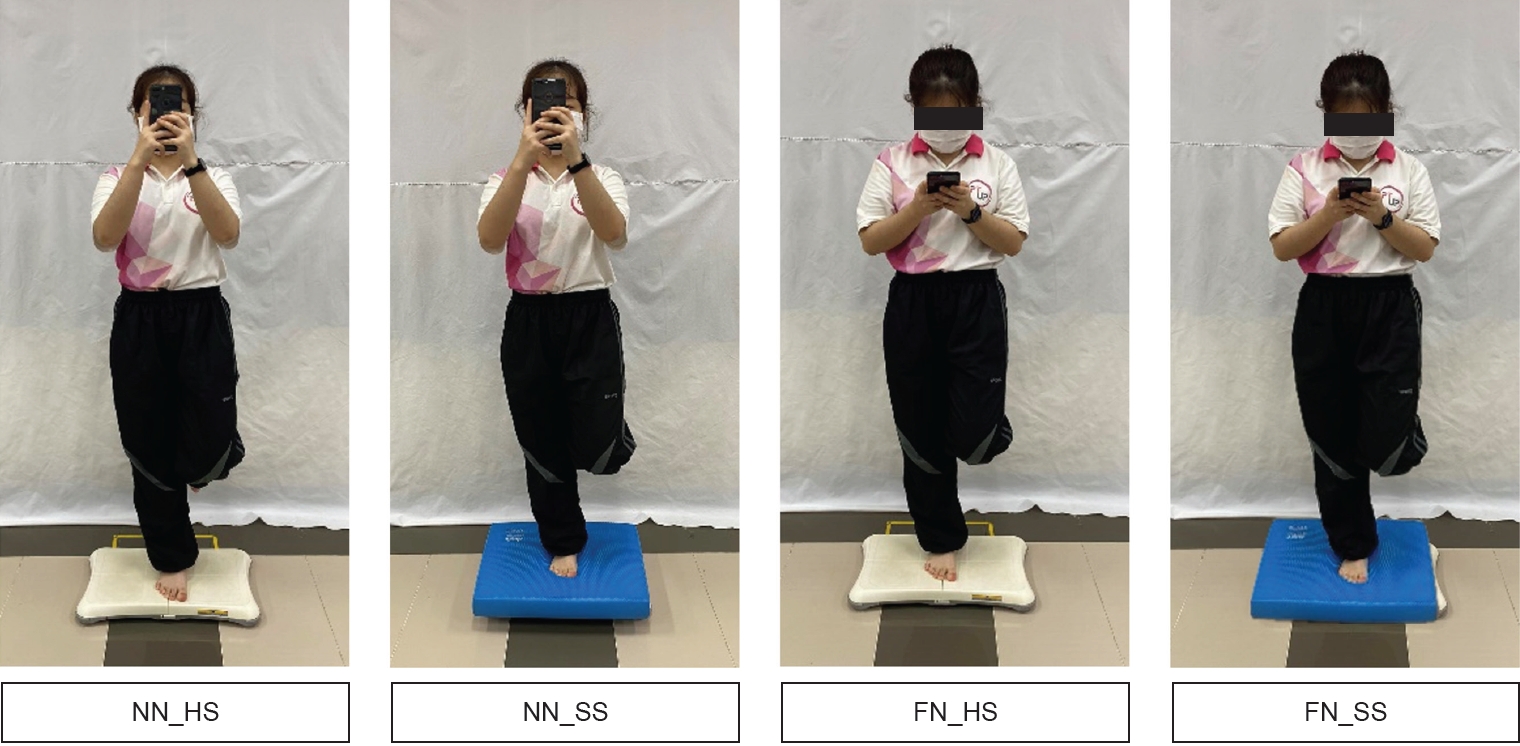
Prior to participating in the study, all participants provided written consent prior to their involvement in the study. Preceding the commencement of the experiment, a random allocation process assigned each participant to one of four distinct conditions. These conditions encompassed smartphone usage in conjunction with neutral neck posture on both hard and soft surfaces, denoted as the NN_HS (neutral neck on hard surface) and NN_SS (neutral neck on soft surface) conditions, respectively (Fig. 3). Additionally, participants were assigned to flexed neck posture on both hard and soft surfaces, FN_HS (flexed neck on hard surface) and FN_SS (flexed neck on soft surface) conditions. This allocation process utilized simple randomization techniques to mitigate potential systematic biases stemming from the sequence of the experimental conditions. Each participant, over separate days, experienced all four conditions.
The postures while using smartphones, neck and shoulder angles, smartphone height, and distance were customized for each participant based on their habitual smartphone usage patterns. This personalization process was aligned with their typical everyday interaction with smartphones, ensuring a tailored fit for each individual. Participants were given three minutes to familiarize themselves with the measurement process, employing a method adapted from Xie et al. (2016) [25]. During each test condition, participants were guided to conduct a single-leg standing test on their dominant leg while continuously typing the English alphabet (A–Z) on their smartphone using both thumbs, while securely holding the device with both hands. Each session had a duration of 1 minute, and a 2-minute break was provided between the two trial sessions. The single-leg standing test began with participants initially standing with both feet on the ground. Subsequently, upon instruction from the researcher, participants were asked to shift their weight to their dominant leg while ensuring both hands retained control of the smartphone, and the non-dominant knee was flexed at a 90-degree angle [21].
NWBB for assessment of postural sway during quiet standing
The NWBB is manufactured using plastic composite material and is outfitted with four load sensors positioned at each corner to measure vertical forces. Data extraction was performed using readily available software, establishing a connection between the NWBB and a laptop via Bluetooth. A Windows-based laptop facilitated data streaming from the NWBB using customized programs and Bluetooth protocol. Sampling of data from the NWBB occurred at a frequency of 30 Hz, a selection based on its similarity to frequencies (10–50 Hz) employed in prior studies [26]. Subsequently, the signal underwent filtering with a 10 Hz cut-off. Before each trial, calibration of the NWBB was executed by applying a known weight (20.4 kg) onto the board [27]. The COP variables were evaluated concerning path length sway, anteroposterior (AP) sway amplitude, and mediolateral (ML) sway amplitude, measured in centimeters. Path length sway measures the total COP travel distance, indicating overall stability. AP sway amplitude quantifies forward-backward displacement, while ML sway amplitude measures side-to-side displacement. High values in these measures suggest instability in their respective directions, providing a comprehensive view of balance [28].
Statistical analysis
The statistical analysis involved the use of IBM SPSS software version 26.0 (IBM SPSS Statistics), with a pre-set significance level (α) of a=0.05. Descriptive statistics, such as means and SDs, were used to showcase the demographic data of the participants. A Shapiro–Wilk test was performed to examine the normal distribution of the variables. After testing for normal distribution and confirming that all variables were normally distributed, we employed an independent t-test to compare body COP sway variables between different groups across each test condition.
Ethical approval
In accordance with the Declaration of Helsinki, all volunteers provided written, informed consent before participating in the study. Additionally, all experimental procedures were conducted following the approval of the Institutional Review Board of the University of Phayao, Thailand (Approval Code No. UP-HEC 1.2/079/66).
RESULTS
Participant demographics and anthropometric data are presented in detail in Table 1. No statistically significant differences (p>0.05) were observed between the control and FHP groups in any demographic or anthropometric variable except for CV angle. The control group exhibited a significantly higher CV angle (mean±SD: 54.46°±3.76°) compared to the FHP group (45.51°±3.57°, p<0.001).
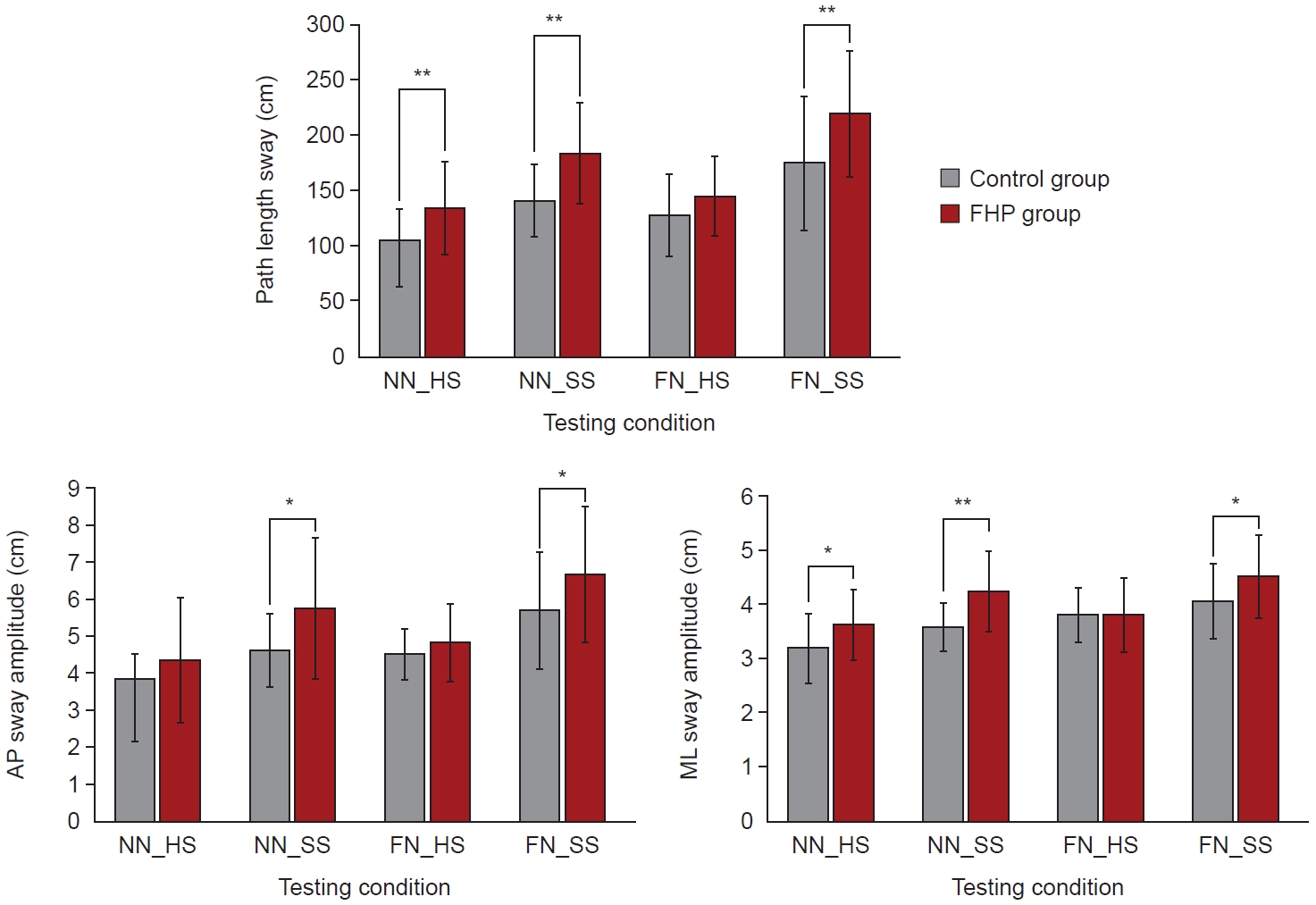
The findings from the NWBB test indicated that the path length sway of the FHP group was notably higher compared to the control group across various posture, with the most significant difference observed in the standing position with a FN_SS, the path length sway was greater in the FHP group than in the control group (184.05±45.87 cm vs. 141.42±33.06 cm). However, in the standing position with a FN_HS, there was no significant difference observed between the FHP group and the control group (145.42±35.40 cm vs. 128.21±36.76 cm) as shown in Fig. 4 and Table 2.
The FHP group exhibited notably higher AP sway amplitude compared to the control group. The most significant difference in AP sway amplitude between the FHP group and the control group was observed in the standing position with a FN_SS (5.73±1.90 cm vs. 4.62±0.99 cm). However, there was no notable difference in AP sway amplitude between the FHP group and the control group in the standing positions with a NN_HS (4.35±1.67 cm vs. 3.85±0.68 cm) and with a FN_HS (4.83±1.03 cm vs. 4.51±0.69 cm) as shown in Fig. 4 and Table 2.
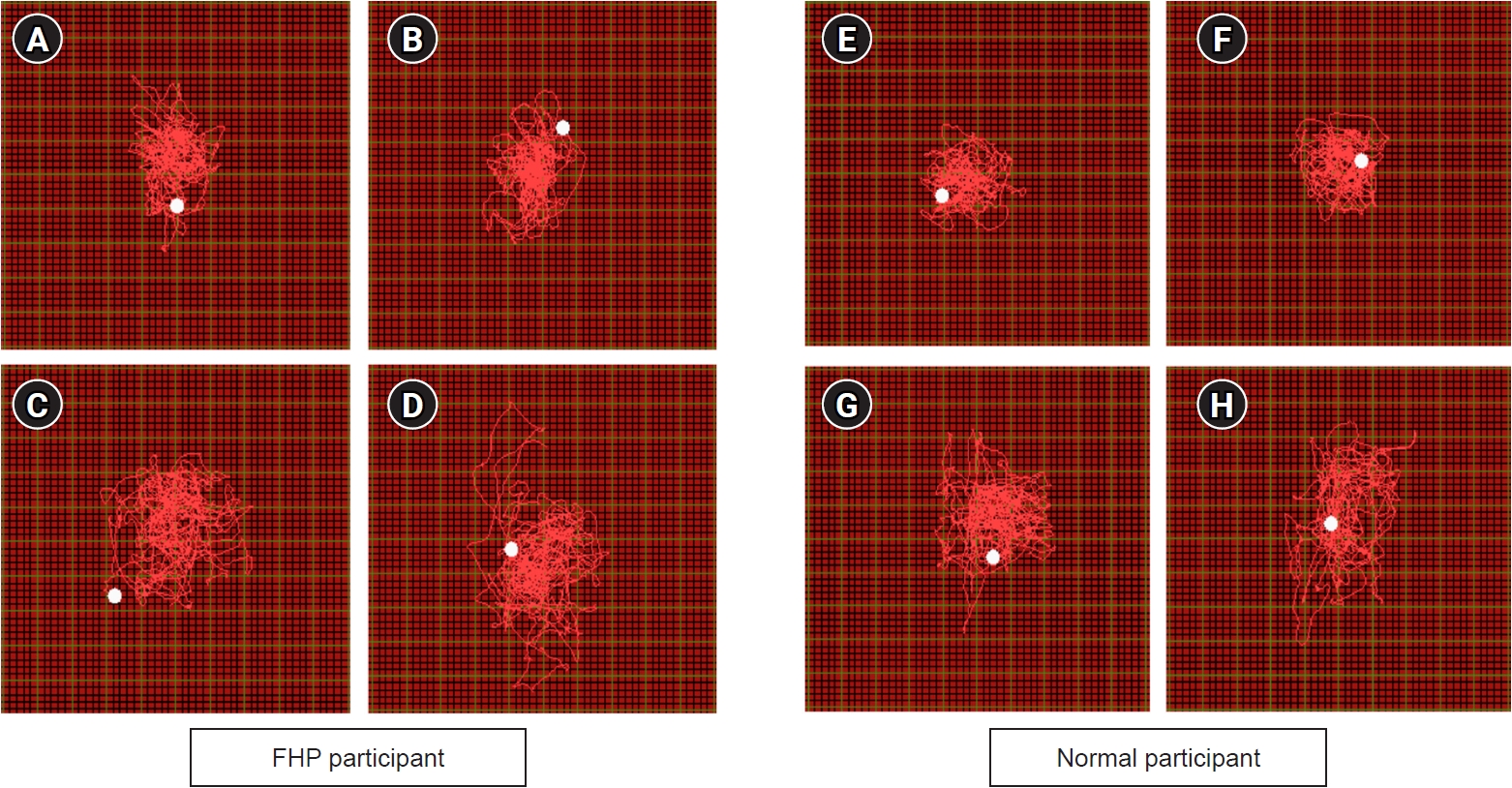
The FHP group displayed notably higher ML sway amplitude compared to the control group across various test positions, except for the standing position with a FN_HS. The most substantial difference in ML sway amplitude between the FHP group and the control group was observed in the standing position with a FN_SS (4.23±0.74 cm vs. 3.58±0.44 cm) as shown in Fig. 4 and Table 2. Moreover, an example of sway trajectories for participants in each group was presented in Fig. 5.
DISCUSSION
The research revealed that individuals with FHP exhibited significantly greater body sway compared to the control group when using smartphones. Notably, distinct variations were observed in path length sway, AP, and ML sway amplitude, particularly evident when maintaining flexed neck positions on a soft surface while engaged with smartphones. These findings highlight the impact of FHP on postural stability, suggesting that the combination of poor posture and smartphone use can exacerbate balance issues, potentially leading to increased risks of falls and musculoskeletal discomfort.
Maintaining balance and postural stability is vital for the overall health and well-being of smartphone users. While smartphone use itself might not directly affect balance or posture, extended periods spent on these devices can result in musculoskeletal issues, spinal misalignment, increased risk of falls, compromised breathing and circulation, muscular fatigue, and even impact psychological well-being [29]. Proper posture during smartphone use can prevent problems like neck strain, back pain, and shoulder discomfort. Overall, prioritizing balance and postural stability during smartphone use is integral to maintaining overall health and averting potential health complications associated with prolonged screen time [30]. FHP, often associated with prolonged smartphone usage, can significantly impact balance, and increase fall risks in healthy smartphone users [30]. When the head protrudes forward from its natural alignment, it alters the positioning of the spine and affects the body’s COG [16]. This misalignment can compromise proprioception, the body’s ability to sense its position in space, leading to instability and difficulties in maintaining balance [11]. As a result, individuals with FHP may experience challenges in equilibrium, especially when standing or moving, thereby increasing the risk of falls or accidents. The disrupted alignment of the spine due to prolonged FHP can negatively affect the body’s coordination and spatial awareness, making it harder for individuals to react appropriately to changes in their environment and increasing the likelihood of losing balance and falling [18,31]. These falls can lead to injuries such as sprains, strains, fractures, or other trauma, particularly when compounded by distracted smartphone use that diverts attention away from the surroundings.
In this study, FHP participants exhibited significantly greater sway compared to the control group across various postures measured by the NWBB. Path length sway and AP sway amplitude showed the most pronounced differences, particularly in the standing position with FN_SS. Notably, no significant sway differences were observed between groups in the FN_HS standing position. ML sway amplitude followed a similar pattern, with FHP exhibiting greater sway in all positions except FN_HS. These findings suggest that FHP participants have greater postural instability during smartphone using, especially in challenging FN_SS postures. Several potential factors contribute to the heightened postural instability observed in individuals with FHP during smartphone use. Firstly, an Altered COG emerges as a significant reason. FHP displaces the COG forward, imposing greater strain on the muscles of the neck and upper back for maintaining equilibrium [32]. Consequently, this increased load makes it more challenging to swiftly respond to postural disturbances induced by smartphone interactions [16]. Diminished proprioception stands as another contributing factor to the postural challenges associated with FHP [33]. The compression of nerves in the neck, a consequence of FHP, interferes with proprioception, the body’s inherent ability to perceive its position in space [34]. This interference leads to a decreased sense of self-awareness regarding body position and movement, thus complicating the adjustment of posture for maintaining balance while engaging with a smartphone [30]. Increased muscle tension is a notable outcome associated with FHP, resulting in the tightening of muscles located in the neck and chest regions [35]. This heightened tension imposes restrictions on the usual range of motion and limits the spine’s flexibility [36]. Consequently, individuals with FHP encounter difficulties in executing subtle postural adjustments necessary for maintaining balance, especially when engaged in smartphone use that involves holding the device in front of the body. The constrained movement caused by this muscle tightness further complicates the body’s ability to adapt and stabilize during such activities.
Engaging in dual-tasking, such as standing on one leg while using a smartphone, impacts postural stability through several key mechanisms. Firstly, attentional resource competition arises from the simultaneous demand for attention in maintaining balance and allocating cognitive resources to smartphone tasks, potentially leading to insufficient resources for balance control and increased instability [37]. Secondly, cognitive engagement can disrupt the automatic postural adjustments triggered during single-leg standing, resulting in delayed or inadequate responses and heightened sway [38]. Thirdly, sensory-motor interference from smartphone use can overload the visual system, causing conflicting signals about body position and movement, hindering effective balance control [37]. Additionally, tasks demanding higher cognitive processing on smartphones increase the mental load, further depleting resources for balance control. Emotional stress induced by dual-tasking can divert attention from balance, exacerbating instability, especially in individuals with existing balance concerns [39]. Moreover, the biomechanical stress of single-leg stance coupled with smartphone usage challenges the musculoskeletal system, intensifying postural instability [40]. These factors collectively contribute to compromised balance control during dual-tasking activities.
One notable finding from the research is the absence of distinctions between groups when employing a smartphone in the FN_HS position. Conversely, in the NN_HS position, differences emerged among groups concerning path length and variables related to ML sway. However, upon comparing these conditions, it became evident that using a smartphone in the FN_HS position resulted in greater sway in all directions compared to the NN_HS position. This suggests that adopting a flexed neck posture while using a smartphone led to deteriorated stability in maintaining posture. The reason behind the lack of difference between the groups in this scenario might be attributed to the possibility that both individuals with a normal posture and those with a FHP experience a similar degree of balance disturbance when in the FN_HS posture. Conversely, the use of smartphone in NN_HS posture might accentuate the contrast between the two groups. Additionally, the shift in the COG of the head, particularly in individuals with FHP, could contribute to these observed differences in postural stability in NN_HS posture.
This study’s limitation lies in its design as a short-term cross-sectional experiment, restricting its capacity to solely elucidate the immediate effects of smartphone utilization on postural stability in individuals with FHP. Nevertheless, while acknowledging this constraint, the findings obtained from this study are likely to offer a representative glimpse into the impact of smartphone use on the balance of individuals with FHP. Thus, despite its short-term nature, the study’s outcomes can still contribute meaningfully to describing the effects of smartphone usage on the balance of individuals dealing with FHP. Future studies in this field could explore longitudinal research tracking prolonged smartphone effects on postural stability among individuals with FHP. Additional constraint of this study is the absence of consideration for the subjects’ neck pain. The research solely focused on including smartphone users with FHP based on the analysis of the CV angle. Not accounting for individuals experiencing neck pain may have influenced the outcomes, potentially leading to distinct results. Future studies should consider including individuals specifically experiencing neck pain alongside FHP to assess potential variations in the effects of smartphone use on postural stability. Another limitation of this study is the absence of an evaluation involving single leg standing without using a smartphone. This restricts our ability to assess the pure effect of FHP on postural stability. Future research should incorporate assessments of single leg standing both with and without smartphone usage to better isolate and understand the specific impact of FHP on balance and stability.
In conclusions, our study assessed balance maintenance using the NWBB across different conditions involving flexed neck postures (FN_HS and FN_SS) and neutral neck postures (NN_HS and NN_SS) on both hard and soft surfaces. The results consistently revealed significantly increased body COP sway lengths in individuals with FHP using smartphones compared to the control group, except in the scenario of flexed neck posture on a hard surface. This suggests that individuals with FHP, while using smartphones, experience notable decreases in balance, particularly in situations involving flexed neck postures on soft surfaces and when multitasking. These findings underscore the potential challenges individuals with FHP may face in maintaining balance during smartphone use in specific postures and environmental conditions. Ultimately, these research implications underscore the importance of further exploration, awareness, and intervention strategies to promote better posture and mitigate balance challenges among smartphone users, especially those with FHP, thereby enhancing overall musculoskeletal health and well-being in the digital age.