Characteristics and Clinical Course of Dysphagia Caused by Anterior Cervical Osteophyte
Article information

Abstract
Objective
To investigate swallowing characteristics of patients with dysphagia caused by anterior cervical osteophytes (ACOs) and compare clinical courses according to treatment options.
Methods
A retrospective analysis of 1,866 videofluoroscopic swallowing studies (VFSS) of patients with ACOs from electronic medical records was performed. Patients with other diseases that could explain the dysphagia were excluded. Dysphagia characteristics and severity and clinical and radiological characteristics of subjects with ACOs were evaluated. Dysphagia characteristics and clinical course were compared among three treatment groups: surgical treatment, swallowing rehabilitation, and conservative treatment.
Results
Subjects were 22 men and 1 woman with a mean age of 78.69±8.01 years. The mean osteophyte thickness was 9.07±3.84 mm. It was significantly thicker in the surgical group than that in other groups (p=0.01). ACOs were most frequently found at C5 level. This level also had the thickest osteophytes. However, videofluoroscopic dysphagia scales (VDS) were not significantly different among the three treatment groups. The pharyngeal phase score of the VDS was significantly higher in the surgical group (p=0.041). Dysphagia severity was decreased significantly in the surgical group at 3 months after the initial VFSS (p=0.004).
Conclusion
The main swallowing characteristics in patients with ACOs were dysphagia features of the pharyngeal phase, including inappropriate airway protection, decreased laryngeal elevation, and reduced epiglottis inversion. When determining treatment options, it may be helpful to consider dysphagia severity at pharyngeal phase and osteophyte thickness.
INTRODUCTION
Spinal osteophytosis is a common disease in the elderly population. More than 75% of people over 65 years old have age-related changes in cervical vertebra anatomy [1]. There are various causes for the development of anterior cervical osteophytes (ACOs). The majority of cervical osteophytes occur due to degenerative diseases. Other causes for the development of anterior osteophytes include diffuse idiopathic skeletal hyperostosis (DISH), failure of surgery, adjacent segmental instabilities after fusion, heterotopic ossification after cervical disc arthroplasty, and posttraumatic instabilities [2,3]. Most of the time, an ACO does not present with any accompanying symptoms. However, prominent ACOs can cause dysphonia, dyspnea, dysphagia, and pain [4]. Dysphagia is the most common presentation of symptomatic ACOs [3]. According to Granville et al. [5], 10.6% of people presenting with dysphagia have cervical osteophytes. According to Utsinger et al. [6], 17% of patients with cervical osteophytosis develop dysphagia.
ACOs could be isolated or diffuse. They are most often idiopathic as a part of the disease entity called DISH [1]. DISH is characterized radiologically by flowing calcification along anterolateral sides of contiguous vertebrae of the spine [7]. Secondary dysphagia due to DISH has been frequently described in case reports [2]. There are no treatment guidelines for dysphagia induced by ACOs. Several cases have described the effect of surgical management on symptomatic osteophytes [3]. However, evidence for surgical approach remains insufficient.
The aim of this study was to analyze swallowing characteristics of dysphagic patients with ACOs and compare clinical courses according to different treatment options.
MATERIALS AND METHODS
Subjects and study design
This was a retrospective study of 1,866 patients who had dysphagia with videofluoroscopic swallowing study (VFSS) at Inje University Haeundae Paik Hospital from April 2014 to December 2017. Eligibility criteria were: (1) patients who had VFSS performed for evaluation of dysphagia and (2) those with ACOs of the cervical spine confirmed by radiologic study. Patients with brain lesions, neuromuscular disease, or other causes that could explain their dysphagia were excluded. A total of 1,866 patients who had VFSS were identified in the electronic medical record (EMR) and reviewed. Twenty-three patients met the eligibility criteria. These 23 patients were enrolled and classified into three groups. Patients who underwent surgery for ACOs were classified into group A (n=4). Those who received swallowing rehabilitation were assigned into group B (n=9) and those who received conservative treatment were classified into group C (n=10). Conservative treatment included diet modification and medications such as muscle relaxants and antiinflammatories [2]. This study was performed according to the Declaration of Helsinki. It was approved by the Institutional Review Board of Inje University Haeundae Paik Hospital (No. 2016-12-013). Subject enrollment and flow are shown in Fig. 1.
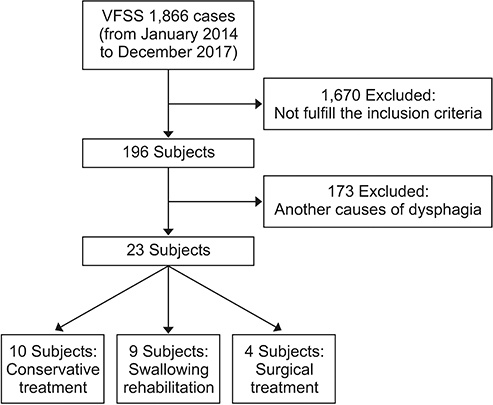
Flow diagram showing subject selection procedures.
Swallowing and ACO assessment
A VFSS was performed by two medical doctors and one occupational therapist. Patients were seated upright on a fluoroscopy chair or wheelchair. The protocol of VFSS in Inje University Haeundae Paik Hospital started with a lateral scout neck image, including cervical spine. The image was taken on the lateral plane and included lips anterior to the vertebrae and the soft palate superior to the 6th cervical vertebra [8]. Barium sulfate powder was used for fluorescence and mixed with either water, liquid diet (water rice gruel), soft diet (rice gruel), or solid diet (rice). Each type of barium diet was then swallowed by the patient. Imaging was then recorded. The anterior-posterior view was also assessed. Two physiatrists analyzed VFSS results. If the patient visibly aspirated on the videofluoroscopy, they did not progress to the next test diet.
In this study, ACO or DISH was well visualized on scout images of VFSS and on plain lateral radiographs of the cervical spine. Radiologic findings of ACO were also assessed by two physiatrists. The affected level(s) and the thickest level of ACO were identified. The thickness of the most prominent ACO was measured. ACOs were classified into three types: segmental, continuous, and mixed [9].
Outcome measurements
Demographic and clinical dysphagia characteristics, dysphagia severity, and VFSS findings of subjects were evaluated. Swallowing characteristics and clinical courses were compared among the three treatment groups. Clinical characteristics related to swallowing were measured using numerical (from 0 to 100) clinical dysphagia scale (CDS) [9]. Dysphagia severity was assessed using the American Speech-Language-Hearing Association National Outcomes Measurement System (ASHA NOMS) swallowing scale and the videofluoroscopic dysphagia scale (VDS). VDS is a numerical scale (from 0 to 100) that measures VFSS findings as objective, quantitative scores directly converted from physiologic parameters of the VFSS [10]. It was created using prognostic factors known to be reliable, objective, and quantifiable predictors of long-term persistent dysphagia after stroke [11]. It has been previously noted that the VDS is a useful scale for quantifying the severity of dysphagia in various disease and age groups [10].
Each parameter of VDS was used to compare VFSS findings. The VDS consisted of two phases: oral phase and pharyngeal phase. Scores and parameters of each phase were compared among the three groups. Temporal parameters such as oral transit time (OTT), pharyngeal delay time (PDT), and pharyngeal transit time (PTT) were also measured and compared. Definitions of above parameters have been published previously [12]. In addition, clinical courses were compared among the three groups using the ASHA NOMS swallowing scale and VDS scores at 3 months after the initial VFSS.
Correlations between treatment options and various characteristics of patients
As mentioned above, subjects were divided into three groups: those who received surgery (group A), patients who participated in swallowing rehabilitation (group B), and those who opted for conservative treatment (group C). Various characteristics suspected to be associated with these treatment options in these dysphagic patients with ACOs were investigated. Patients’ demographics, clinical swallowing characteristics, radiologic findings, dysphagia severity, and VFSS findings were used to analyze their correlations with treatment options.
Statistical analysis
Data analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). Sociodemographic, osteophyte-specific, and swallowing characteristics of subjects were analyzed using descriptive statistics that included frequency, percentage, and mean±standard deviation. To compare gender, clinical dysphagic symptoms, comorbidity, and osteophyte level, Pearson chi-square and Fisher exact tests were used. When comparing three groups, one-way ANOVA or Kruskal-Wallis test was used depending on the normality of data distribution. If necessary, post-hoc analysis (Scheffe) was done. Spearman rank correlation analysis was also performed to identify correlation of treatment options with other characteristics. All tests were two-tailed and a p-value of less than 0.05 was considered statistically significant.
RESULTS
Demographic and clinical characteristics of patients
Demographics and clinical characteristics of ACO patients are summarized in Table 1. This study included 22 men and 1 woman. Their mean age was 78.69±8.01 years (range, 62–89 years). Average dysphagia symptom duration was 96.91±205.19 days. In group A, 3 patients had DISH-induced ACO and 1 patient had cervical osteoarthritis (OA). In group B, DISH was observed in 5 patients whereas cervical OA was noted in the other 4 patients. Likewise, in group C, 3 patients had DISH whereas the remaining 7 patients had cervical OA. No significant difference in the etiology was found among the three groups (p=0.298).
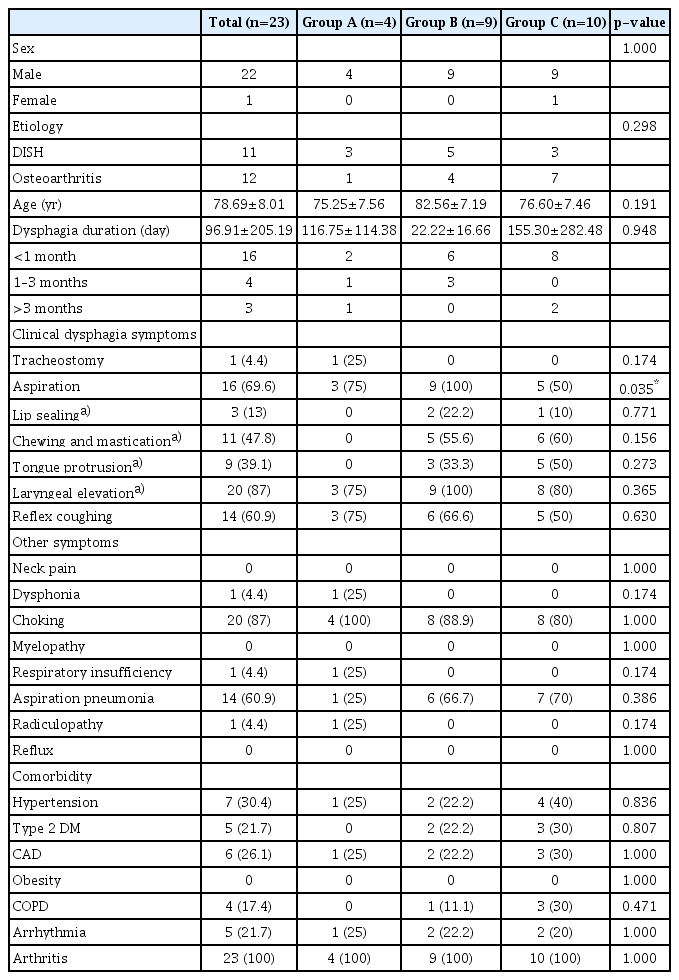
Demographics and clinical characteristics of dysphagic patients with ACO
The most common CDS findings included inadequate laryngeal elevation (87.0%), aspiration (69.6%), and reflex coughing (60.9%). Lip sealing and tongue protrusion in oral function were intact in 87.0% and 60.9% of subjects, respectively. In the surgical group, all subjects maintained their oral function. The most commonly associated symptom was choking, followed by aspiration pneumonia. There was no significant intergroup difference in age, gender, symptom duration, or other combined symptoms and comorbidities. The most common comorbid conditions were arthritis, hypertension, type 2 diabetes mellitus, and coronary artery disease. All subjects had arthritis.
Radiologic findings of ACO
Of 23 patients, C5 (n=20) was the most commonly affected level, followed by C6 (n=18), and C4 (n=16). In group A, all patients had osteophytes at levels C3, C4, and C5. In groups B and C, C5 and C5-6 levels were the most commonly affected. There were no intergroup differences in most affected levels. The level with the thickest osteophytes was C5 (n=8), followed by C6 (n=6) and C4 (n=5). Level C4 was the thickest level in group A. It had a significant intergroup difference (p=0.009). The mean osteophyte thickness was 9.07±3.84 mm (range, 3–18 mm). Average thicknesses of groups A, B, and C were 13.13 mm, 7.83 mm and 8.55 mm, respectively. Osteophytes in group A were significantly thicker than those in the other groups (p=0.01). Overall, 9 cases were classified as segmental type ACOs, 7 cases as continuous type, and 7 cases as mixed type ACOs. The type of osteophytes and the number of affected levels showed no significant intergroup difference (Table 2).

Radiologic findings of ACO
Dysphagia severity and swallowing characteristics in patients with ACO
The mean CDS score showed no significant inter-group difference (45.00±26.77 in group A vs. 43.44±14.81 in group B vs. 32.5±15.1 in group C). With all patients included, mean ASHA NOMS swallowing scale and VDS scores were 2.17±1.58 and 40.04±10.06, respectively. Dysphagia severity showed no significant inter-group difference in ASHA NOMS swallowing scale (2.25±0.83 in group A vs. 1.44±1.25 in group B vs. 2.90±1.64 in group C) or VDS (53.13±6.66 in group A vs. 49.22±9.35 in group B vs. 44.85±14.37 in group C). However, the pharyngeal phase score of the VDS showed significant intergroup difference (p=0.041). The pharyngeal phase score of group A was higher than that of group C. The most common VFSS finding included penetration (100%), decreased laryngeal elevation (91.3%), and reduced epiglottis inversion (87.0%). In group A, all patients showed incomplete upper esophageal sphincter (UES) opening in addition to the above findings, with residue in the valleculae and pyriform sinuses. Incomplete UES opening had a significant intergroup difference (p=0.016). However, temporal parameter such as OTT, PDT, or PTT showed no significant inter-group difference (Table 3).

Dysphagia severity and swallowing characteristics in ACO patients
Clinical courses in dysphagic patients with ACO
Of the 23 ACO patients, 4 underwent surgical intervention. After surgery, 3 patients who could not swallow anything safely were able to eat orally. The remaining patient improved from level 4 to level 7 in ASHA NOMS swallowing scale. In all three groups, there were no significant intra-group differences in ASHA NOMS swallowing scale after treatment. However, group A showed a trend toward statistically significant improvement (p=0.059). Followup evaluation using ASHA NOMS swallowing scale demonstrated a significant inter-group difference (p=0.009). The score of group A was increased more than that in the other two groups. Dysphagia severity according to ASHA NOMS swallowing scale after treatment also showed inter-group differences between group with surgical treatment and groups without surgical treatment (p=0.047).
Ten patients underwent follow-up VFSS at 3 months after the initial procedure. The mean change in VDS score was 27.0±6.36 for group A, 1.9±8.61 for group B, and 1.5±6.87 for group C, showing significant inter-group difference (p=0.014). In post-hoc analysis, group A showed significant change in the follow-up VDS score than the other groups (Table 4). Two patients in the surgical group underwent follow-up VFSS. After surgical treatment, their pharyngeal phase scores were decreased by 16.5 and 31.5, respectively. Based on VDS item, the amount of residue in the pyriform sinus was decreased. Moreover, aspiration and penetration showed improvement.
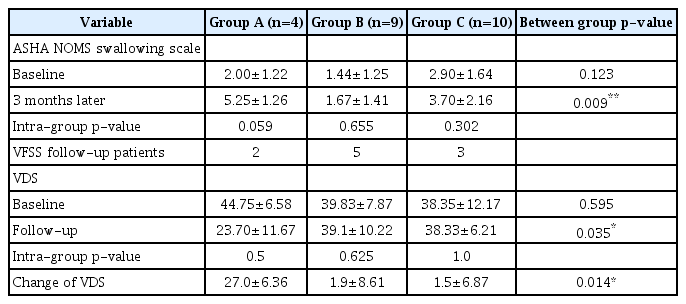
Comparison of dysphagia severity at 3 months after the initial VFSS
Correlations between treatment options and various characteristics in patients with ACO
C3 osteophyte level, pharyngeal phase score of VDS, inadequate bolus formation, reduced epiglottis inversion, and incomplete UES opening showed significant correlations with treatment options. The correlation between pharyngeal phase score of VDS and treatment options was the largest, followed by incomplete UES opening and C3 osteophyte level (Table 5).

Correlations between treatment options and various characteristics
DISCUSSION
In this study, 22 of 23 patients (96%) were males. Their mean age was 78.7 years. A meta-analysis study of 204 cases by Verlaan et al. [13] has reported that the maleto-female ratio of ACO incidence is 6.1:1 and the average age is 68.9 years. Kim et al. [14] have reported that ACOs occur more frequently in men and that the average age at onset is 66 years. This is generally consistent with our study demographics. ACOs were reported in 2.9% to 4.1% of adults in Korea [14]. Its prevalence is known to increase with age [14]. Seidler et al. [15] have found that the dysphagic symptom severity increases with age. Because life expectancy is increasing, the prevalence of dysphagia due to ACOs may also increase in the coming decades [14].
Spondylosis is a common finding in the aging cervical spine [16]. ACOs can be a result of such degenerative disorders of the cervical spine. Indeed, in this study, all participants had arthritis. Symptomatic degenerative changes of the cervical spine affect approximately 75% of the population aged more than 60 years [16]. Therefore, older male patients with unexplained dysphagia may need to evaluate cervical spine for possible ACOs.
The main findings of this study were that swallowing characteristics of dysphagic patients with ACOs showed pharyngeal phase dysphagia including penetration, decreased laryngeal elevation, and reduced epiglottis inversion. The surgical group had a significant higher pharyngeal phase score of VDS than the other groups. Moreover, in the surgical group, the thickest and most affected level of ACO were at higher level of the cervical spine and their ACOs were significantly thicker than the other two groups.
Although some studies have suggested various mechanisms to account for ACO-induced dysphagia, the exact mechanisms remain unclear. Dysphagia due to ACO is most commonly associated with anterior osteophyte formation at C3-5 levels. This might be due to the fact that the normal epiglottic tilt lies over the laryngeal inlet at these levels [13]. In this study, all patients in group A had ACOs at C3-5 levels and showed reduced epiglottis inversion, decreased laryngeal elevation, and penetration on VFSS findings. According to Di Vito [17], bolus deflects off directly into the open larynx because of the shelf formed by an anterior osteophyte at C3-5 levels. This has been reported to cause direct aspiration [17]. Seidler et al. [15] have reported that osteophytes at C3-4 and C4-5 levels are associated with aspiration during swallowing due to restriction of the epiglottic closure. This type of aspiration was more common in patients of group A who had ACOs at higher cervical spine levels. In contrast, residue retention with possible post-swallow aspiration is often found in patients with osteophytes in lower cervical spine levels (C5-6, C6-7) [15]. Osteophytes at the C6-7 level can cause esophageal impingement or obstruction [17]. Group C had more osteophytes at C6-7 level. However, esophageal impingement or obstruction was not detected on VFSS. This suggests that osteophytes might not be thick enough to cause such conditions.
According to Strasser et al. [18], aspiration is rare in patients with osteophytes <10 mm. They found that clinically relevant obstruction of the pharynx occurred from about 12 to 15 mm osteophyte thickness. Seidler et al. [15] have reported that osteophytes >10 mm in the anteriorposterior length could lead to symptoms related to dysphagia. In our study, osteophyte thickness in group A was 13.13±2.26 mm, which was significantly thicker than that in other groups. The mean osteophyte thickness was 9.07±3.84 mm (range, 3–18 mm). These findings were consistent with results of other studies. The thickness of the osteophyte can affect the epiglottic tilt or direct aspiration into the larynx. It can also cause physical obstruction of the esophageal lumen. In addition, increased thickness may increase the incidence and severity of symptoms such as choking and aspiration. In the present study, the surgical group showed significantly higher scores in pharyngeal phase of VDS than the other groups. This suggests that laryngeal dysfunction along with aspiration may influence the decision to undergo surgical treatment.
There is no consensus about proper ACO treatments at this time. Most case reports and studies have reported improvements in dysphagia symptoms within 6 weeks after surgical treatment. von der Hoeh et al. [2] have reported improvements in VFSS findings and dysphagia symptoms in all their six patients after surgery. Flynn [19] have reported improvement of dysphagia symptoms in 28 of 30 patients after surgical resection of ACOs. In our study, the surgical group showed significant improvements in their dysphagia severity compared to the other treatment groups. The swallowing rehabilitation group did not show significant improvement in dysphagia severity. This might be due to the small sample size, short follow-up duration after swallowing rehabilitation, and difficult structural changes in osteophytes. However, swallowing rehabilitation has been suggested as a treatment option because neuromuscular strengthening and diet modification can help improve patients’ symptoms [20-22].
Based on EMR review, patients with thick ACO and definite aspiration were recommended to undergo surgery. In the surgical group, 3 out of 4 patients were referred to a neurosurgeon after VFSS in the rehabilitation department while the other patient underwent orthopedic surgery recommended by the otolaryngologist. In the swallowing rehabilitation group, 2 out of 9 patients refused surgery but underwent rehabilitation and 2 patients were unable to undergo an operation due to the presence of comorbidities. The remaining 5 patients were determined to conduct swallowing rehabilitation by an internist. Moreover, we compared VDS total score (40.50±6.47, 39.30±10.30) and VDS pharyngeal phase score (32.75±7.96, 33.90±8.32) of patients who were recommended for surgical treatment and those who were determined to initially undergo rehabilitation. There was no statistically significant difference (p=1.0 and p=0.905, respectively). In the conservative treatment group, 1 of 10 patients refused the recommended surgical treatment and 7 patients refused the swallowing rehabilitation. Two patients were isolated. Hence, rehabilitation was not performed. For patients with dysphagia caused by ACO, surgical indication or treatment method has not been established yet. Therefore, selection of treatment option by patient might have influenced the final decision of the treatment method.
Characteristics associated with treatment options in dysphagic patients with ACOs were analyzed. ACOs at C3 level had positive correlations with treatment options. Those in the more active treatment groups such as patients who underwent surgery and swallow rehabilitation had frequent alterations on the upper cervical spine, especially at the C3 level. A systematic review of 204 cases by Verlaan et al. [13] has elucidated that the most affected vertebrae are C3, C4, and C5 known to be associated with epiglottic tilt. Based on the study by Bartalena et al. [23], VFSS shows epiglottis impingement at C3–C4 level which alters the pharyngeal phase of swallowing and leads to laryngeal penetration. von der Hoeh et al. [2] have also reported that most surgeries are performed at C3–C4 level. Osteophytes at the C3–C5 level may cause inflammation of the anterior spinal soft tissue at the cricopharyngeal opening, thus inhibiting the opening of the UES [17]. It has been reported that the upper esophageal sphincter opening width is significantly increased, along with an improvement of hyoid movement after surgical treatment of ACOs [3]. Consistent with other studies, all patients in the surgical group of the present study had ACOs at C3–C5 level and showed laryngeal penetration, decreased laryngeal elevation, reduced epiglottis inversion, and incomplete UES opening. Moreover, ACO was significantly thicker in the surgical group. Therefore, upper cervical spine alterations, severity of the pharyngeal dysphagia, and ACO thickness might need to be considered when deciding for appropriate treatment options.
Although beneficial effects of surgical removal have been reported, surgical management of ACOs in dysphagia patients is still being debated. Post-surgical soft tissue edema and laryngeal nerve damage can occur. Therefore, there is a chance that surgery can actually degrade swallowing [24]. If there are long-term progressive bone formation and irreversible surrounding tissue changes, it is impossible to completely resolve dysphagia through surgery [25]. Therefore, it is important to establish a proper surgical indication. In an attempt to assist with decisionmaking, correlations between treatment options and various factors were analyzed. If patients’ pharyngeal dysphagia and incomplete UES opening are severe, they are more likely to undergo active treatment such as surgery and swallow rehabilitation rather than with conservative treatment.
This study has several limitations. First, it was conducted retrospectively using EMR of subjects. For this reason, selection bias could not be ruled out. Second, the number of subjects was small which limited the study’s validity. Third, VFSS follow-up was not performed for all patients after treatment. Therefore, it could not fully evaluate changes of VFSS findings.
In conclusion, the main swallowing characteristics in patients with ACOs were dysphagia features of pharyngeal phase including inappropriate airway protection, decreased laryngeal elevation, and reduced epiglottis inversion. When deciding on a treatment option, considering the severity of dysphagia, specifically at the pharyngeal phase, and the overall osteophyte thickness might be helpful.
Notes
No potential conflict of interest relevant to this article was reported.