INTRODUCTION
Stroke causes significant changes in the urinary system, and various urinary symptoms appear. Urinary incontinence is a known predictor of moderate to severe stroke [1], and the prevalence of lower urinary tract symptoms (LUTS) after a stroke was higher in stroke patients (64%) than in the general population (34%) [2].
An overactive bladder (OAB) is defined by the International Continence Society for patients with urinary urgency, with or without urge incontinence, and with urinary frequency and nocturia, but in the absence of infection or obvious neoplastic, metabolic, or other pathologies [3]. OAB is related to physical and mental health as well as to other symptoms, including skin breakdown due to leakage, sleep disturbance, fall-related injuries, depression, prolonged hospital stays, admission to a nursing home, and lower quality of life (QOL) [4,5]. Stroke is known as a risk factor for OAB [6], and the OAB prevalence is 12.4%ŌĆō53.1% in elderly adults [7,8,9]. However, little is known about the prevalence of OAB in stroke patients. Itoh et al. [10] found that of 500 stroke patients, 28% had OAB.
Although OAB is considered to be highly prevalent, its etiology remains unknown. The pathophysiology of OAB is complex and involves both peripheral and central nervous system factors. An increased afferent activity, decreased capacity to process afferent information, decreased suprapontine inhibition, and increased sensitivity to contraction-mediating transmitters are all potential central nervous system causes of OAB that can be induced by stroke.
OAB is an embarrassing condition that interferes with social functioning and daily living activities. However, caregivers and medical staff can overlook a diagnosis of OAB, which may result in an undertreatment of its symptoms. In contrast, urinary incontinence that obviously lowers the health-related QOL (HRQOL) of patients and caregivers can easily be noticed and treated [11]. Although a large proportion of stroke patients seem to have low HRQOL due to OAB symptoms, few studies have investigated the effect of OAB symptoms on stroke patients' HRQOL, especially during rehabilitation.
To understand the effect of OAB symptoms in stroke patients' HRQOL, we conducted a questionnaire-based survey at baseline and at 3 months of follow-up and analyzed the results together with clinical data.
MATERIALS AND METHODS
Patients and study design
We screened patients who had experienced a stroke and who were admitted to the rehabilitation center between March 2014 and May 2016. The inclusion criteria were as follows: (1) the patient was diagnosed with stroke, (2) the lesion was confirmed via brain magnetic resonance imaging or computed tomography imaging, (3) more than 1 month passed after the onset of the stroke, (4) the patient's age was between 20 to 80 years, (5) the patients maintained intact cognitive function and were able to understand and complete the questionnaire. Patients with urinary tract infection, chronic renal failure, pelvic organ prolapse, urethral stricture, prostate-related operation history, prostate specific antigen (PSA) of more than 4.0 ng/mL, history of bladder cancer, severe medical comorbidities, and cognitive impairment disorder were excluded. Patients who were unable to void spontaneously or whose postvoid residual urine volume was greater than 300 mL [12], who had OAB symptoms or urinary incontinence from 6 months before onset, and who did not complete the questionnaire were also excluded.
A total of 30 stroke patients (14 female, 16 male) were enrolled in this study and signed the informed consent forms. Participants were divided into two groups: an OAB group and non-OAB group according to the Overactive Bladder Symptom Score (OABSS), which is a screening tool for OAB symptoms. The OAB group was defined with an urgency score of 2 or more and a total score of 3 or more, in accordance with previous studies [13].
The participants were surveyed to evaluate their HRQOL, and their performance was assessed twice: at the time of enrollment and 3 months later after the baseline survey. A transrectal ultrasonography (TRUS) was performed, and the PSA level was assessed in men. All patients were subjected to uroflowmetry to evaluate the urine flow rate.
The study was approved by the Institutional Review Board of the National Rehabilitation Center (IRB No. NRC-2014-01-006), and all participants gave written informed consent.
Questionnaire
OABSS was developed to screen patients with OAB symptoms and to evaluate the severity of OAB symptoms [14,15], and it was recorded in all patients. It consists of four questions covering the daytime frequency, nocturia, urgency, and urgency incontinence, with maximal scores of 2, 3, 5, and 5, respectively. Since urinary urgency is the core symptom of OAB, the OAB group was defined with an urgency score of 2 and total OABSS score of 3 or more [13].
We conducted the survey to evaluate the HRQOL using the Short Form 36 health survey (SF-36) version 2. SF-36 evaluates the following 8 physical and mental health areas: physical functioning (PF), physical role functioning (RP), bodily pain (BP), general health (GH), vitality (VT), social role functioning (SF), emotional role functioning (RE), and mental health (MH). Each of the 8 areas was scored on a scale of 0ŌĆō100, with a higher score indicating better subjective health. These scores were then calculated from the questionnaires responses as previously described. The physical component summary (PCS) and mental component summary (MCS) measures are calculated from these 8 scales using algorithms recommended by the instrument developers [16]. This study was conducted with permission from QualityMetric Inc., Lincoln, RI, USA.
In addition, the International Prostate Symptom Score (IPSS), incontinence quality of life (I-QOL), and Overactive Bladder Questionnaire (OAB-Q) were conducted to identify urinary symptoms.
Clinical data and functional status score
At the time of enrollment, we measured the prostate volume using TRUS in men to rule out benign prostate hyperplasia (BPH), which is very common in elderly men. Patients suspected by an urologist of having BPH were excluded. All patients were examined via uroflowmetry to evaluate the urine flow rate, and clinical information was collected, including types and lesion of stroke, onset of stroke, underlying hypertension, diabetes, and other cardiovascular diseases. The performance scores, such as Function Ambulation Category (FAC), Modified Rankin Scale (MRS), Modified Barthel Index (MBI), and Mini-Mental State Examination (MMSE), were assessed by clinical doctors at baseline and at 3 months later.
Statistical analysis
The baseline characteristics were compared between the OAB and non-OAB groups. For the comparison, t-test and chi-square test were used. We used Mann-Whitney U-test to compare two groups at baseline and at 3 months of follow-up. A longitudinal analysis was assessed by a Wilcoxon signed-rank test. We used a correlation analysis and a multivariate regression to assess whether the OAB symptoms were associated with 3-month MCS. The variables obtained through baseline surveys were selected using the backward elimination method during a multiple regression analysis. The statistical significance was confirmed using a goodness-of-fit test and a significance test of the regression coefficient. The statistical significance was considered when p-value was Ōēż0.05, and the data were analyzed with the SPSS ver. 21 statistical package (IBM, Armonk, NY, USA).
RESULTS
Participant characteristics
From March 2014 to May 2016, a total of 39 stroke patients signed a consent form, but 9 refused the last survey. The mean age of 30 participants was 58.9 years, and the mean onset duration of stroke was 4.6 months. We divided subjects into two groups: OAB group (n=12) and non-OAB group (n=18). The general characteristics and demographic information of the 30 subjects and the differences between the two groups are presented in Table 1. Only one patient had aphasia, and this patient was in the non-OAB group.
OABSS was evaluated twice. Three patients reported aggravation of OAB symptoms over 3 months, and there was no urinary tract infection or other urinary related events. In the initial evaluation, 4 patients were using anticholinergics, and there was no restriction to change medication in this study. All 4 patients maintained the medication, and 1 patient showed deterioration in the OABSS score. After the initial evaluation, 4 patients started taking anticholinergics due to OAB symptoms, and the rest of the patients in the OAB group were symptomatic but did not take medication.
HRQOL and OAB symptoms
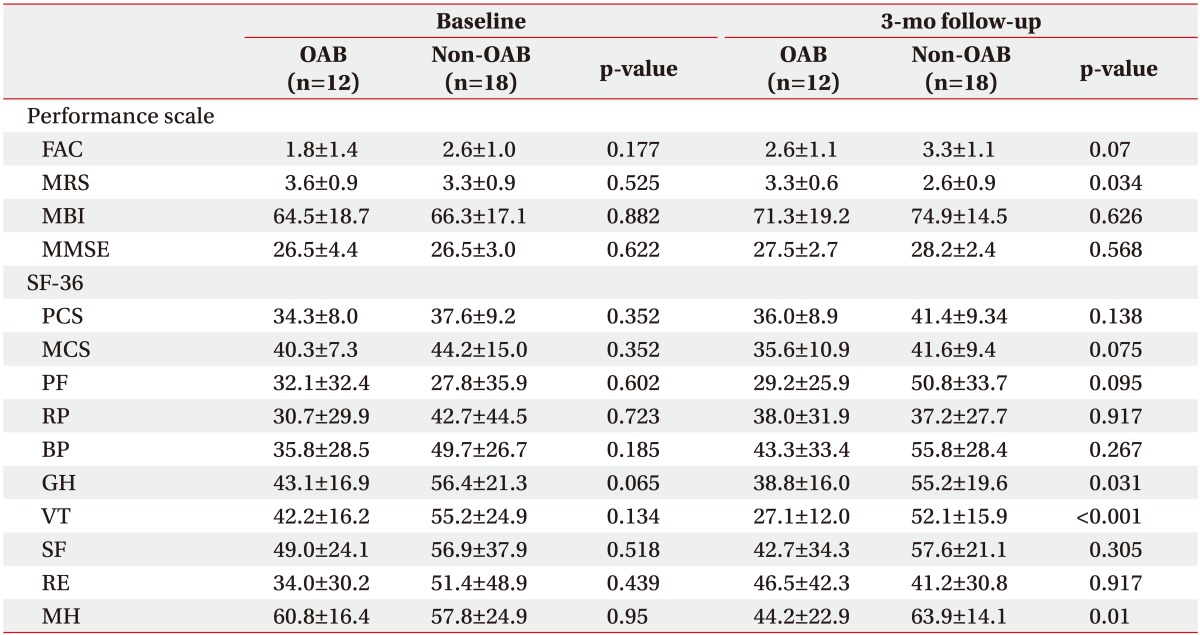
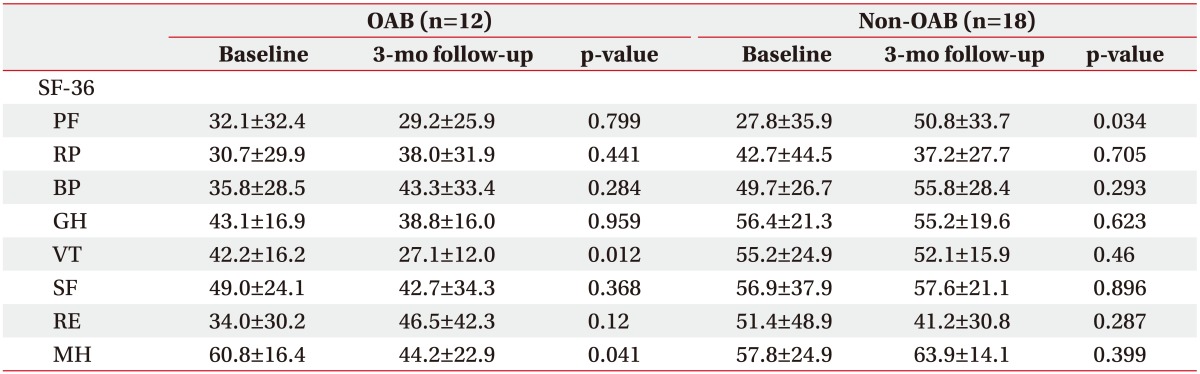
Looking at SF-36, which presents the general HRQOL of the patients, both PCS and MCS scores showed no difference between the OAB group and non-OAB group at both baseline and at 3-month follow-up (Table 2). In a longitudinal analysis, the MCS score showed a marginal decrease over time only in the OAB group (p=0.05) (Table 3, Fig. 1). As we look into the subareas of SF-36, no difference was seen between the two groups at baseline, but the general health, vitality, and mental health areas showed a lower score in the OAB group compared to the non-OAB group at 3 months of follow-up (Table 2). The vitality and mental health areas had a significant decrease in scores over 3 months in the OAB group (p=0.011 and p=0.041, respectively) (Table 3). In a multivariate regression, the presence of OAB symptoms was significantly associated with lower MCS scores at 3 months (B=-8.15, p=0.034) (Table 4). Therefore, the OAB symptoms seem to have a negative effect on the mental component of the HRQOL. Other subareas of SF-36 showed no difference at 3 months of follow-up compared to that at baseline, but the physical functioning area showed an improvement at 3-month follow-up (p=0.03).
The I-QOL total score and HRQOL score of OABQ showed no difference between the two groups (p=0.54 and p=0.37 respectively), but the questions regarding lower urinary tract symptoms in OABQ showed a significant difference between the two groups (p<0.001).
Performance scale scores and OAB symptoms
In the non-OAB group, all patient performance scales showed an improvement over time (all p<0.02). However, in the OAB group, the FAC and MBI showed an improvement (p=0.04 and 0.005, respectively), but MRS and MMSE did not improve significantly (p=0.15 and p=0.20, respectively) (Table 2). At 3-month follow-up, the MRS scores were lower in the non-OAB group (p=0.034), indicating less disability.
Assessment of urinary symptoms
At the baseline, the use of anticholinergics and the results of the uroflowmetry and TRUS showed no differences between the OAB and non-OAB groups (Table 1). The international prostate symptom score showed a significant difference in both storage and voiding scores between the two groups at baseline, but there was no longitudinal change over 3 months in both the OAB group (p=0.34) and non-OAB group (p=0.86).
DISCUSSION
We prospectively assessed the HRQOL and performance scale scores at baseline and at 3 months of follow-up of post-acute stroke patients. Patients who had OAB symptoms seemed to have greater burden in the mental aspect of HRQOL at the 3-month follow-up. Moreover, there is a possibility that the OAB symptoms affect the physical and cognitive performance of stroke patients.
Urinary incontinence has been reported to be a predictor of mortality and poor functional outcomes after a stroke [1]. Urinary incontinence negatively affects the QOL in the general population, especially in patients with stroke who have neurologic deficits such as dysphagia, visual field defects, motor weaknesses, and cognition and language impairments [17]. In addition to urinary incontinence, OAB symptoms also cause considerable inconvenience to stroke patients. However, previous studies have mainly focused on the prevalence of urinary incontinence after stroke. Only a few studies were carried out for OAB symptoms, such as urinary urgency, frequency, and nocturia, and these studies used a simple questionnaire for community-based stroke patients [2,17,18,19]. Since there was no study on the effect of OAB symptoms during rehabilitation treatments, we found that the vitality and mental health scores of SF-36 exhibited a significant decrease over 3 months in the OAB group, and the presence of OAB symptoms was significantly associated with a lower MCS score at 3 months of follow-up. The OAB symptoms seem to have a negative effect on the mental component of the HRQOL. Although this regression model explains only 22% of the variance in the MCS, it can add strength to our hypothesis.
Several prognostic factors for OAB have been reported in the general population. For men, comorbidities, including arthritis, depression, heart disease, hypertension, mobility limitations, neurological conditions, recurrent urinary tract infection, BPH, and prostatitis, are suggested to be predictors of OAB [7,20]. BPH associated with LUTS prevalence rates ranged from 50%ŌĆō75% among 50 years and older men to 80% among 70 years and older men [21]. Therefore, an objective evaluation of lower urinary tract symptoms due to BPH is necessary to minimize bias in elderly men. We underwent TRUS by an urologist to assess the prostate in male participants.
Itoh et al. [10] analyzed questionnaires on 500 stroke patients. OAB was identified in 28% of patients, with lower HROQL scores in both the physical and mental components of SF-8. The elderly and male patients were also associated with OAB. Compared with a previous study, we found no difference between the two groups in the initial HRQOL evaluation, but HRQOL scores were lower in patients who had OAB symptoms only in the mental component at the 3-month follow-up. Moreover, we can see the change in HRQOL by evaluating SF-36 twice in 3 months.
We found that MRS and MMSE showed less of an improvement in the OAB group than in the non-OAB group, and the physical functioning score of SF-36 showed a significantly higher score at 3 months of follow-up, compared to baseline (p=0.034). We might infer the possibility that OAB symptoms may affect the performance in patients with stroke. Therefore, a further study with more patients and a longer follow-up period is needed to prove this hypothesis.
This study had several limitations. Although this was a prospective study, it was conducted in a single institution with a small number of patients. Only patients with an adequate cognitive level to respond to the questionnaire and with the bladder control to participate in uroflowmetry were included in this study. In addition, due to the small number of patients, it is difficult to analyze the relationship between the changes in HQOL and OAB symptoms according to the use of medication. Therefore, larger prospective investigations are required to overcome these limitations and to determine the precise effects of OAB symptoms after stroke.
In addition to the negative impact of the OAB symptoms on the HRQOL of stroke patients, the detection and proper treatment of OAB symptoms in stroke patients should be encouraged to improve their HRQOL.
In conclusion, our findings indicate that OAB symptoms have negative effects on the physical and cognitive performance of stroke patients, and as the recovery process progresses, the burden of OAB symptoms may become more pronounced on HRQOL, especially regarding the mental component. Therefore, OAB symptoms should not be overlooked, and they need to be treated in stroke patients.