Neurodevelopmental Disorders of Children Screened by The Infantile Health Promotion System
Article information
Abstract
Objective
To perform an in depth evaluation of children, and thus provide a systematic method of managing children, who after infantile health screening, were categorized as suspected developmental delay.
Method
78 children referred to the Developmental Delay Clinic of Ilsan Hospital after suspected development delay on infantile health examinations were enrolled. A team comprised of a physiatrist, pediatrician and pediatric psychiatrist examined the patients. Neurological examination, speech and cognitive evaluation were done. Hearing tests and chromosome studies were performed when needed clinically. All referred children completed K-ASQ questionnaires. Final diagnoses were categorized into specific language impairment (SLI), global developmental delay (GDD), intellectual disability (ID), cerebral palsy (CP), motor developmental delay (MD) or autism spectrum disorder (ASD).
Results
72 of the 78 patients were abnormal in the final diagnosis, with a positive predictive value of 92.3%. Thirty (38.4%) of the 78 subjects were diagnosed as GDD, 28 (35.8%) as SLI, 5 (6.4%) as ASD, 9 (12.5%) as MD, and 6 (7.6%) as normal. Forty five of the 78 patients had risk factors related to development, and 18 had a positive family history for developmental delay and/or autistic disorders. The mean number of abnormal domains on the K-ASQ questionnaires were 3.6 for ASD, 2.7 for GDD, 1.8 for SLI and 0.6 for MD. Differences between these numbers were statistically significant (p<0.05).
Conclusion
Because of the high predictive value of the K-ASQ, a detailed evaluation is necessary for children suspected of developmental delay in an infantile health promotion system.
INTRODUCTION
Development is the process in which a child acquires daily living skills and continually adapts itself to different situations. It can be defined as the maturation of the central nervous system and as the structuralization of cognitive, psychological and behavioral functions interlocked with physical, biological and environmental factors.1 Developmental disorders, which include both developmental delay and deviation, refer to children who are mentally or physically inhibited for their ages; these problems affect 5 to 10% of children.2,3 Developmental disorders are caused by various factors, but can be prevented or minimized through early detection and intervention. Accordingly, many studies have been conducted to detect developmental disorders in their early stages. As a result, various diagnostic tools have been developed and applied.4-6
The Ages and Stages Questionnaire (ASQ) is suitable for cases of suspected developmental disorders, and has the merit of being inexpensive and easy-to-answer.7 The ASQ is intended for children aged 60 months or less, and is completed by the parents. It consists of 5 domains (communication, gross motor, fine motor, problem solving and personal-social) and each domain consists of 6 questions. The questionnaires are classified according to age. Points obtained from each domain are compared to a cutoff threshold of two standard deviations and the cutoff threshold is used to distinguish normal from suspected developmental delay.
In Korea, the Korean Ages and Stages Questionnaire (K-ASQ) has been standardized and applied clinically.8 In particular, the K-ASQ has been used to screen for developmental delays in the national child health checkup program, which commenced on November 15, 2007. Children suspected of a developmental delay on the K-ASQ questionnaire are referred to specialized clinics.9 However, a nationwide system managing suspected developmental delay children has not yet been established in Korea, and studies on evaluation of such referred children are lacking.
This study analyzed results of an in-depth evaluation of children referred to our hospital after being categorized as 'suspected developmental delay' or 'reevaluation required' on the Infantile Health Promotion System. We wanted this study to provide a basis for establishing a clinical management system for such children.
MATERIALS AND METHODS
Subjects
This study included 78 children, 62 boys (79.4%) and 16 girls (20.5%), who were referred to our hospital after being categorized as 'suspected developmental delay' or 'reevaluation required' in the infantile health promotion system between January 2008 and March 2011. Their average age was 27.2 months (9-61 months).
Methods
Examinations were performed by physiatrists, pediatric psychiatrists and pediatric neurologists according to a diagnostic protocol. In addition to physical and neurologic examinations, speech, language and cognitive evaluations were performed. When necessary, hearing tests, brain MRI scans and chromosome tests were performed and the children were subsequently categorized using etiological and clinical diagnoses.
K-ASQ: Due to the long time interval between referral and the actual visit to our clinic, the K-ASQ survey was re-conducted, again according to the child's current age. The questionnaire was filled out by parents or foster parents. The cut-off threshold was defined as a score that was below two standard deviations from the mean. Cases that fell short of the threshold were classified as 'suspected developmental delay', and scores that came close to the threshold were classified as 'reevaluation required.'
Speech and language evaluation: Speech and language evaluations were performed using the Sequenced Language Scale for Infants (SELSI) or the Preschool Recep tive-Expressive Language Scale (PRES).10,11 Language delay was defined as a disparity of more than two standard deviation between linguistic and chronological age on SELSI, or when more than one year of delay was detected on PRES.
Cognitive evaluation: Cognitive evaluation was performed using the Bayley Scales of Infant Development II (BSID-II), the Korean Wechsler Preschool and Primary Scales of Intelligence (K-WPPSI) or the Korean Wechsler Intelligence Scales of Children-III (K-WISC III).12,13
Diagnostic classification: The children were diagnostically classified as specific language impairment (SLI), global developmental delay (GDD), intellectual disability, cerebral palsy, motor developmental delay (MD) or as autistic spectrum disorder (ASD). SLI was diagnosed when the developmental delay was confined to language, and not to cognition or motor and social function. In addition, performance intelligence had to be 85 or higher on the Wechsler scales, and the psychomotor developmental index (PDI) 70 or higher on the Bayley scale. Intellectual disability was diagnosed when the intelligence quotient was less than 70, and borderline intelligence was also categorized as intellectual disability. The Bayley test was used as a substitute when the Wechsler test could not be performed and a diagnosis of GDD was included in the intellectual disability group. ASD included cases with problems in language and social function, and included autism, pervasive developmental disorder and Asperger syndrome. Children who did not show pervasive problems in development and who were not diagnosed with cerebral palsy, but were having significant problems in motor function, were diagnosed with MD after taking into account motor function domains of the Bayley test.14
Statistical analysis: Statistical analyses was performed using SPSS PC 16.0. The chi-square test was used to analyze differences in K-ASQ domains amongst the diagnostic groups (GDD, SLI, ASD and MD). Intergroup characteristics were analyzed by one-way ANOVA. The significance level was defined as p-values that were less than 0.05.
RESULTS
It took an average of 6.5 days (0-24 days) for the children to visit our hospital's Developmental Delay Clinic after abnormalities on the Infantile Health Promotion System screening and subsequent referral.
Of a total of 78 children, 45 (57.6%) had risk factors related to development. Among them, 34 (43.6%) had neonatal risk factors such as premature birth, jaundice, meconium aspiration, septicemia and multifetal gestation. The other 11 (14.1%) had perinatal risk factors including pre-eclampsia, gestational diabetes and drug use. In particular, 11 (15.2%) were born prematurely, and 18 (23.1%) had a family history of developmental delay, language delay, mental retardation or autism.
Of 78 children referred to this hospital, 72 were ultimately diagnosed with neurodevelopmental diseases and 6 were concluded to be normal. Thus, the positive predictive value of the K-ASQ was 92.3%. Of the final diagnoses, GDD accounted for the highest proportion (30; 38.4%), followed by SLI (28; 35.8%), MD (9; 11.5%) and ASD (5; 6.4%) (Fig. 1).

The final diagnosis of children referred for suspected developmental delay. GDD: Global developmental delay, SLI: Specific language impairment, MD: Motor developmental delay, ASD: Autism spectrum disorder, NL: Normal.
The five domains of the K-ASQ among the four diagnoses were analyzed. Communication, gross motor and personal-social domains among the four groups showed statistically significant differences (p<0.05) (Table 1) whereas fine motor and problem solving domains did not (Table 1). Of children with ASD, 100% showed abnormalities in the communication domain, in contrast to a mere 11% in the MD group. However, approximately 80% of children with MD and only 10% of children with SLI showed abnormal scores in the gross motor domain. In the personal-social domain, the ASD group, the SLI group and the MD showed abnormal scores in 80%, 20% and 20% of the children, respectively.
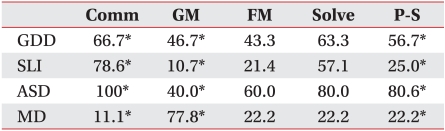
Abnormal Pattern of K-ASQ Scores According to the Diagnosis
For each diagnosis, a score defined by the number of abnormal domains was calculated. The ASD group got the highest score, 3.6, followed by the GDD group with 2.7, the SLI group with 1.8 and the MD group with 0.6. Thus, there were significant intergroup differences (Table 2) (p<0.001).
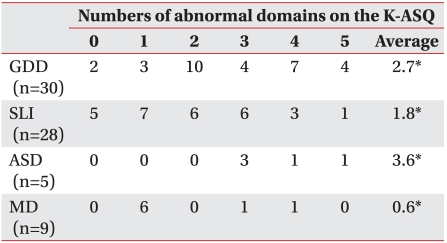
Numbers of Abnormal Domains According to the Diagnosis
DISCUSSION
Early detection and intervention are crucial in preventing and minimizing developmental disorders. Developmental disorders may occur at any stage of development, and thus it is advisable for the child to undergo checkups periodically.15-18 Many studies have been conducted to develop screening tools for high-risk children,4-7 and the Ages and Stages Questionnaire (ASQ) and the Denver Developmental Screening Test (DDST) have been used as standardized tools in Korea.4,8 In particular, the K-ASQ does not require training and is easily completed within 10 to 15 minutes by parents. Furthermore, its accuracy in identifying high risk children with developmental delay has been proven through many studies.3,4,19-23 As a result, the K-ASQ has been used as a screening tool in the infantile health promotion system, a nationwide project that commenced on November 15, 2007. This study includes data of children referred to our hospital within three years since the commencement of this nationwide project.
In this study, most of the children referred showed abnormal results after an in-depth evaluation at our clinic, and thus a high positive predictive value of K-ASQ was identified. Skellern et al. reported that the positive predictive value of the ASQ reached 40%, but Lindsay et al. reported that it reached 85 to 92%.15,24 In this study the positive predictive value was 92.3%. However, the value measured in this study, might be overstated to some extent in that a checkup was not done for all the children judged abnormal by the initial K-ASQ done during the Infantile Health Promotion System screening. Moreover, parents may have chosen to forgo referrals and further evaluations despite abnormal results on the initial K-ASQ. However, the results of this study imply that it is necessary to perform in-depth evaluations on children judged abnormal on screening tests such as the K-ASQ.
In this study, over half of the children referred to our hospital were found to have risk factors, unlike normal children. In particular, 15.2% of the children were born prematurely, which is a high percentage when compared to the 3.93% rate of infants in the general population that were born prematurely between 1995 and 2007.25 In common with previous studies, this study re-confirmed the high incidence of neurodevelopmental disorders in cases with existing risk factors such as premature birth.
Not many studies have been conducted on the family history of neurodevelopmental disorders. In Korea, a study reported that approximately 4.3% of children with ASD had a positive family history.26 In this study, 23.1% of the children had a positive family history where a parent, sibling or relative was diagnosed with motor function or language delay, which implies that developmental disorders are to some extent heritable.
In this study, the four diagnoses showed different but distinctive abnormalities in the five domains of the K-ASQ. Many of the children showing global delays in development such as those in the GDD or ASD groups, were found to have abnormal results in all five domains of the K-ASQ. Children with selective delays such as SLI and MD group members, tended to have language and gross motor problems, respectively.
This study has limitations in that it did not include the whole cohort that underwent the Infantile Health Promotion System screening program. Due to this limitation, sensitivity and specificity K-ASQ could not be calculated. In this regard, a post management system of those previously screened under the Infantile Health Promotion System needs to be established and further epidemiologic research or cohort studies through registration of children with risk factors is necessary.
CONCLUSION
This study shows that many of the children referred after Infantile Health Promotion System screening were found to have neurodevelopmental disorders. Early detection and intervention is crucial in improving prognosis in children with neurodevelopmental disorders. Accordingly, it is clinically important to accurately diagnose, through in-depth medical evaluations, children with suspected developmental delay. Furthermore, establishing a post-test management system after Infantile Health Promotion System screening is essential.