Comparison of Clinical Characteristics Between Patients With Different Causes of Vocal Cord Immobility
Article information

Abstract
Objective
To analyze the clinical characteristics between neurogenic and non-neurogenic cause of vocal cord immobility (VCI).
Methods
The researchers retrospectively reviewed clinical data of patients who underwent laryngeal electromyography (LEMG). LEMG was performed in the bilateral cricothyroid and thyroarytenoid muscles. A total of 137 patients were enrolled from 2011 to 2016, and they were assigned to either the neurogenic or non-neurogenic VCI group, according to the LEMG results. The clinical characteristics were compared between the two groups and a subgroup analysis was done in the neurogenic group.
Results
Among the 137 subjects, 94 patients had nerve injury. There were no differences between the neurogenic and non-neurogenic group in terms of demographic data, underlying disease except cancer, and premorbid events. In general characteristics, cancer was significantly higher in the neurogenic group than non-neurogenic group (p=0.001). In the clinical findings, the impaired high pitched ‘e’ sound and aspiration symptoms were significantly higher in neurogenic group (p=0.039 for impaired high pitched ‘e’ sound; p=0.021 for aspiration symptoms), and sore throat was more common in the non-neurogenic group (p=0.014). In the subgroup analysis of neurogenic group, hoarseness was more common in recurrent laryngeal neuropathy group than superior laryngeal neuropathy group (p=0.018).
Conclusion
In patients with suspected vocal cord palsy, impaired high pitched ‘e’ sound and aspiration symptoms were more common in group with neurogenic cause of VCI. Hoarseness was more frequent in subjects with recurrent laryngeal neuropathy. Thorough clinical evaluation and LEMG are important to differentiate underlying cause of VCI.
INTRODUCTION
Vocal cord immobility (VCI) is defined as various spectrum of motion impairment in the vocal cord. Although hoarseness is the main symptom in VCI, dysphonia, odynophonia, dysphagia, chronic cough, and laryngospasm can also occur [12]. Visual inspection by a laryngoscopy and electrophysiologic study, such as laryngeal electromyography (LEMG) can help to differentiate the neurogenic and non-neurogenic causes of VCI [34].
The LEMG technique was first introduced by Weddel et al. [5], and needle electrode insertion in small muscles of larynx with assistance of laryngoscopy or in-surgery was first reported in 1950s [678], followed by the standardized percutaneous electrode insertion technique [9]. LEMG is not only helpful in diagnosing neuromuscular disorder in the larynx [101112], but it can also be used in botulinum toxin or hyaluronic acid injection in vocal cord [1314].
In the process of first diagnosing VCI, various systemic diseases can be suspected from the symptoms. Viral or bacterial infections can attribute to post-infectious neuropathies [1516] and a wide spectrum of malignancies or tumors present as a paralysis. Also, VCI can be seen in systematic neurologic diseases such as myasthenia gravis, Charcot-Marie-Tooth disease, and multiple sclerosis [2]. With LEMG results, it aids to select other diagnostic tests and determine timing and type of treatments. Furthermore, LEMG results are useful in predicting negative outcomes and their findings can alter definitive treatments [17]. It is important to diagnose VCI of neurogenic causes and to affect treatment and prognosis. However, there are few research studies regarding the association between the clinical characteristics in VCI and LEMG results.
The aim of this study was to analyze the clinical characteristics between neurogenic and non-neurogenic cause of VCI patients. Furthermore, the researchers tried to compare the clinical characteristics between neurogenic and non-neurogenic VCI patients by the difference of the LEMG findings.
MATERIALS AND METHODS
Subjects
The researchers retrospectively reviewed clinical data of patients who underwent LEMG from the Department of Physical Medicine and Rehabilitation in Korea University Anam Hospital. A total of 137 patients, who underwent LEMG due to clinical symptoms of VCI or abnormal findings in laryngoscopy, were enrolled from January 2011 to December 2016. Motion abnormalities including vocal cord hypomobility or glottic insufficiency were considered as abnormal findings in the laryngoscopy [2]. All the patients who complained symptoms of dysphagia or were suspected to be at risk of aspiration carried out a videofluoroscopic swallowing study (VFSS). Penetration or aspiration was concluded by VFSS findings and the researchers used an 8-point penetration-aspiration scale (PAS) [18]. All subjects were assigned to either the neurogenic or non-neurogenic group, according to the LEMG results. The clinical characteristics were compared between the two groups and a subgroup analysis was done in neurogenic group.
Laryngeal electromyography
Before LEMG, all subjects filled out a questionnaire about their status of suspected vocal cord palsy. Along with questionnaire, general characteristics, clinical symptoms of subjects were collected. Physical examinations including tongue deviation, palpable neck mass, laryngeal elevation, gag reflex was also performed. During the LEMG, a pillow was placed behind the subjects' neck in supine position and the neck was extended. In this position, the researchers indicated thyroid cartilage and cricoid cartilage as surface landmarks of the larynx (Fig. 1).
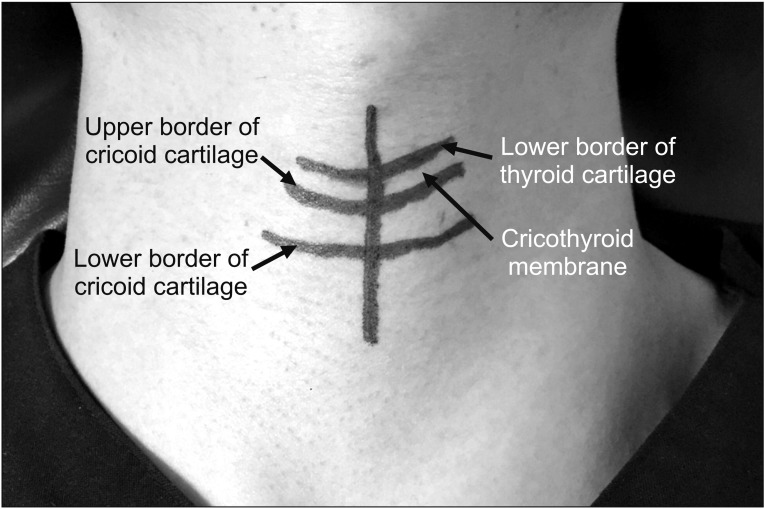
Surface landmark of larynx is illustrated. We drew line to indicate lower border of thyroid cartilage, upper and lower borders of cricoid cartilage, midline of cricothyroid membrane.
LEMG was performed by a single electromyographer (S. Pyun) using a Sierra Wave instrument (Cadwell Industries, Kennewick, WA, USA) and needle EMG was done with a 26-gauge (0.46-mm diameter), 5-cm long monopolar needle electrode. Sweep speed was 10 ms/div and sensitivity was 200 µV/div. Needle EMG was performed in bilateral two small intrinsic muscles of the larynx: the cricothyroid and thyroarytenoid muscles. The cricothyroid is innervated by the superior laryngeal nerve (SLN) and produces tension and elongation of the vocal cord. The needle electrode was inserted into the skin tangentially to the upper border of the cricoid cartilage, superiorly, and laterally [19]. In order to activate the cricothyroid muscle, the subjects were asked to make ‘e’ sound and to produce a high pitch as much as possible [20]. The thyroarytenoid is innervated by recurrent laryngeal nerve (RLN) and helps to reduce tension of the vocal cords during speech to decrease pitch. The needle electrode was inserted into the skin and the cricothyroid membrane. As the electrode passed the membrane, its direction was changed to 20° laterally and 45° superiorly or proximally [19]. In order to activate the thyroarytenoid muscle, subjects were asked to hold their breath after deep inspiration [20]. The researchers considered neurogenic VCI to be present with findings that abnormal spontaneous activities in the muscle at rest, polyphasic motor unit potentials, decreased, or reduced recruitment patterns [32122].
Statistical analysis
Statistical analysis was performed using SPSS Statistics ver. 20 software (IBM, Armonk, NY, USA). Significance was determined when the p-value was less than 0.05. Nominal and categorical variables were expressed with absolute number and relative frequencies. Chi-square test and multinomial logistic regression analysis were used to investigate the association between nominal and categorical variables. Continuous variables were analyzed by an independent t-test comparing the laryngeal neuropathy and normal groups. In the sub-group analysis, continuous variables were analyzed by analysis of variance (ANOVA).
RESULTS
Among the 137 subjects, 94 patients had nerve injury in RLN, SLN or both nerves, and other 43 patients had normal findings in LEMG. About one-fourth of the neurogenic VCI was idiopathic. When excluding idiopathic origin, 50% of the other patients had trauma or intubation history. Neurogenic VCI occurred commonly after treatment of malignancy including thyroid, parathyroid, lung, pancreas, and esophagus. Most malignancies are associated with lymph node metastasis or an invasion near the neck. Viral infection such as herpes zoster, Epstein-Barr virus, cerebellopontine angle mass, and stroke in the medulla also generated neurogenic VCI in some patients (Table 1). Most of the neurogenic VCI patients were treated with conservative therapies such as humidification, mucolytics, voice rest, and positional training initially. After conservative management, 34 patients received injection laryngoplasty, and 16 patients showed improvement of subjective symptoms. Steroid pulse therapy and voice therapy were considered as additional treatment options.
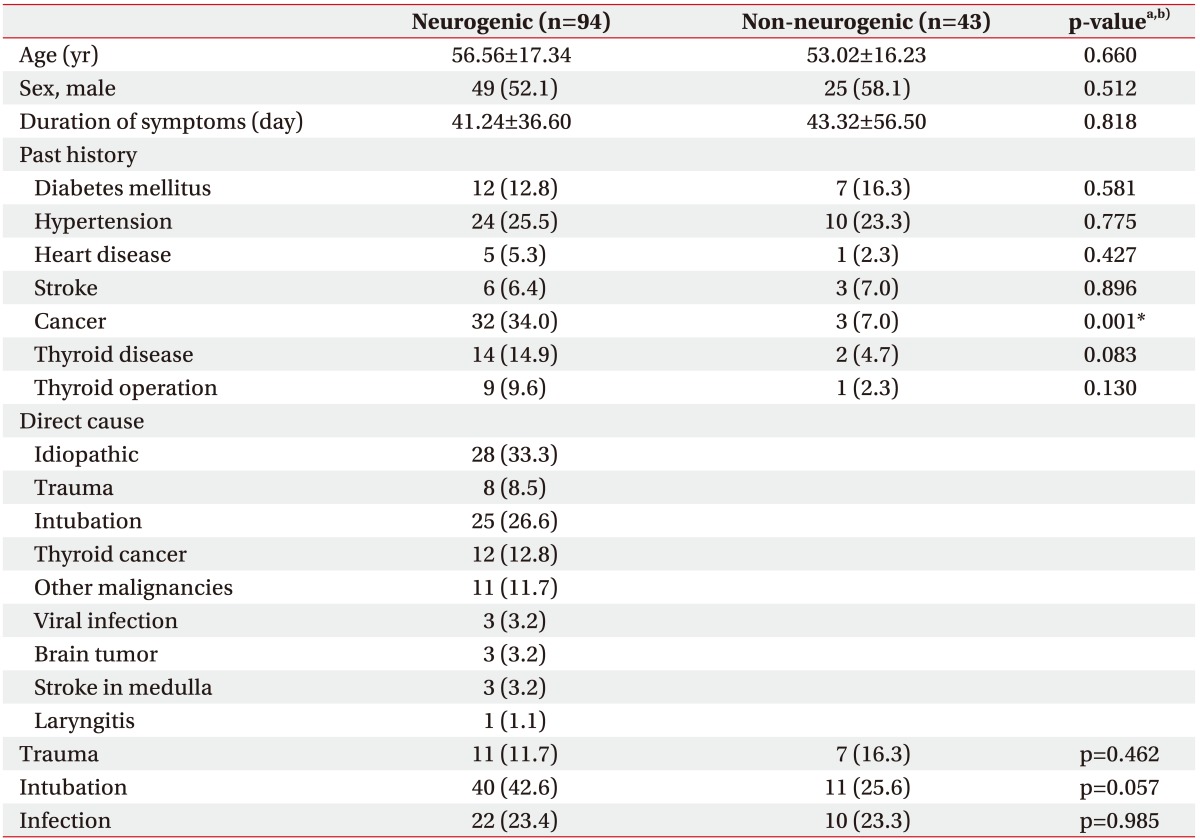
Comparison of general characteristics between neurogenic and non-neurogenic group (n=137)
Comparison between neurogenic and non-neurogenic group
There were no significant differences between the neurogenic and non-neurogenic group in terms of demographic data and premorbid events. However, there was significantly higher tendency associated with cancer history in the neurogenic group than non-neurogenic group (p=0.001) (Table 1). In clinical findings, impaired high pitch ‘e’ sound and aspiration symptoms were more frequent in the neurogenic group and sore throat was more common in the non-neurogenic group (p<0.05) (Table 2).

Comparison of clinical characteristics between neurogenic and non-neurogenic group (n=137)
Subgroup analysis in neurogenic group
Results of subgroup analysis in neurogenic cause of VCI are presented in Table 3. Thyroid operation and infection history showed a correlation between three groups (p<0.05), however there were no significant differences between the RLN and SLN groups. Demographic data, underlying disease, and premorbid events except thyroid operation and infection history were also not different between recurrent laryngeal and superior laryngeal groups (Table 3). Hoarseness had significant correlation between the three groups (p=0.034) and was significantly higher in patients with recurrent laryngeal neuropathy than superior laryngeal neuropathy (p=0.018).

Comparison between RLN and SLN groups (n=94)
Subgroup analysis according to lesion location confirmed by LEMG
A total 91 patients completed a laryngoscopy, of which 88 patients showed abnormal findings in the laryngoscopy. Among the 88 patients, 31 patients showed no abnormal findings in LEMG, 3 patients showed no correlation between laryngoscopy and LEMG findings in terms of lesion location. Therefore, 54 patients (61.4%) showed a correlation in site of lesion between the two examinations.
Because the whole neurogenic VCI patients did not complete laryngoscopy, the researchers divided three groups according to lesion location through LEMG findings. There was significant correlation between the three groups about intubation history and aphonia (p<0.05). However, no significant differences were detected when the researchers compared the right and left VCI groups. All the other variables showed no significant correlation between three groups (Table 4).
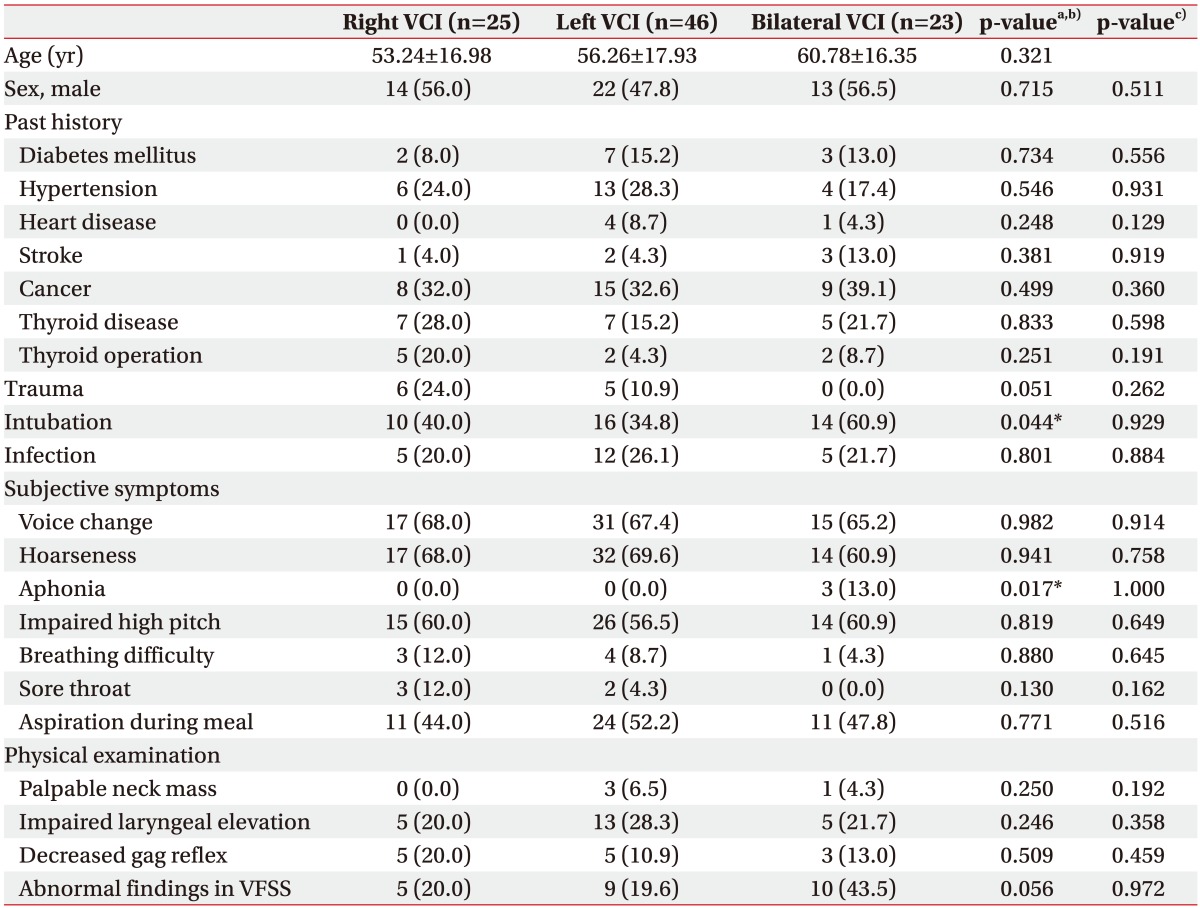
Comparison according to lesion location confirmed by laryngeal electromyography (n=94)
DISCUSSION
In this study, the researchers analyzed clinical characteristics in patients with neurogenic and non-neurogenic causes of VCI. In the neurogenic group, impaired high pitched ‘e’ sound and aspiration symptoms were more common than the non-neurogenic group. Furthermore, hoarseness was more frequent in subjects who had recurrent laryngeal neuropathy.
Patients with VCI usually have one or more laryngeal nerve injuries and it can make inadequate closure or insufficiency of the glottis. These abnormalities are associated with breathing difficulty, dysphonia, and vocal fatigue. Also, neurogenic VCI can occur secondary to systemic disease, malignancy, and surgical interventions around the neck and thorax [2]. The surgery including thyroidectomy, esophagectomy, and lung resection can result in RLN injury due to anatomical course of RLN [23242526]. In this study, cancer history was more common in the neurogenic VCI group than the non-neurogenic VCI group.
The cricothyroid muscle is a key muscle in control of voice frequency, thus superior laryngeal neuropathy can cause poor vocal quality such as vocal cord asymmetry and acoustic aperiodicity [27]. On the other hand, SLN injury had no significant influence on glottal configuration and function in some previous studies [28]. Therefore, accurate diagnosis is important for a favorable treatment outcome of VCI [1729]. In this study, the most common symptoms of both neurogenic and non-neurogenic VCI group were voice change and hoarseness. The 58.5% and 39.5% of neurogenic and non-neurogenic VCI groups had impaired high pitched ‘e’ sound, respectively. High pitched sound was known to be associated with the cricothyroid muscle innervated by SLN [20]. Among the 55 patients with impaired a high-pitched sound in the neurogenic group, 25 patients had superior laryngeal neuropathy or both laryngeal nerve injuries (67.5%). However, impaired high-pitched sound was also common in patients with recurrent laryngeal neuropathy (52.6%). The recurrent laryngeal neuropathy is common in traumatic neurolaryngological lesion. Injury of RLN lead to flaccid ipsilateral vocal cord and it can lead to dysphonia or aphonia, hoarseness and aspiration into trachea [30]. Therefore, vocal cord paralysis can lead to impaired high-pitched sound due to a weak, breathy voice, inability to raise the volume of the voice, and the sensation of running out of air while speaking. In the subgroup analysis, hoarseness was significantly higher in patients with recurrent laryngeal neuropathy. Mild and persistent hoarseness can be detected as the only initial symptom of the patients with compression of RLN [31]. Therefore, recurrent laryngeal neuropathy should be suspected in patients who complain of sudden voice change and hoarseness.
Aspiration risk increased by 37%–50% in the patients with VCI [32] and dysphagia is common in VCI with SLN and/or RLN injuries [33]. Consistent with previous studies, 42.3% of the total VCI patients complained of aspiration during a meal, and the frequency was higher in the neurogenic VCI group than the non-neurogenic VCI group in this study. There was some controversy with the correlation of RLN and aspiration. Swallowing difficulty is not common in patients with only RLN injury [34], but, several reports argued that aspiration can happen in unilateral RLN paralysis [3033].
In this study, abnormal VFSS findings, including penetration and aspiration, were reported in 21.1% of patients with only the recurrent laryngeal neuropathy group. Internal branch of the SLN have association with swallowing, laryngeal closure, and respiratory rhythm [35]. However, there were no patients with SLN injury that showed abnormal VFSS findings. In this study, the researchers enrolled 9 patients in only superior laryngeal neuropathy group, smaller than other groups. These patients were younger (mean age, 45.6 years) and showed lesser underlying diseases than RLN injury group. Also, no abnormal spontaneous activities with mild or chronic neuropathy patterns were detected in 66.7% of patients in SLN injury group. Because of these factors, the researchers could not conclude correlation of RLN, SLN with aspiration exactly in this study.
Many patients complained of pain and discomfort during LEMG. It is difficult to test because of problems in sampling small laryngeal muscles and interfering signals from neighboring muscles [22]. This test needs enough skillfulness to examine. Because of that, some clinicians omitted LEMG in VCI patients occasionally. Nevertheless, with neurologic, pathophysiologic results from LEMG, researchers can diagnose neurologic VCI, neuromuscular disease in larynx and determine the appropriate therapy method. Many authors consider LEMG to be an important tool and recommend its clinical use in patients with suspected VCI [3637].
Limitations of our study were small sample size and retrospectively collected data. There were some findings not consistent with previous studies such as the relationship between dysphagia and SLN. The researchers also could not get the patients' whole information about prognosis because of loss of follow-up and missed medical records. A larger sample size with a prospective study will be needed for adequate statistical analysis and to investigate the clinical outcomes during the long-term follow up period in VCI patients.
In the patients with suspected vocal cord palsy, impaired high pitched ‘e’ sound and aspiration symptoms were more common in a group with neurogenic cause of VCI than a non-neurogenic group. Hoarseness was more frequent in subjects with recurrent laryngeal neuropathy than superior laryngeal neuropathy subjects. Thorough clinical evaluation and electrodiagnostic study of laryngeal muscle are important to differentiate the underlying cause of VCI.
ACKNOWLEDGMENTS
This work was supported by the National Research Foundation of Korea (NRF) funded by the Korea government (No. 2016R1A2B4009206).
Notes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.