Which Factors Unexpectedly Increase Depressive Symptom Severity in Patients at the End of a Cardiac Rehabilitation Program?
Article information
Abstract
Objective
To investigate predictors of depressive symptom aggravation at the end of a cardiac rehabilitation (CR) program.
Methods
The design of the study was retrospective. The administrative data were obtained from the database of the CR department of a heart hospital in Iran. The demographic and clinical information of 615 CR patients between January 2000 and January 2010 was analyzed using binary logistic regression analysis.
Results
The results showed that 10.7% of the patients completed the CR program with aggravated depressive symptoms. After adjustment for gender, age, and pre-intervention depression score, lower education level (p<0.05) and smoking (p<0.01) were significant predictors of increased depressive symptoms at the end of the program. Our model variables could explain 6% to 13% of the dependent variable variance.
Conclusion
The results suggest that targeting patients who are less literate or who smoke could allow for taking the required measures to prevent or control depression at the end of a CR program. It is suggested that future studies consider other variables.
INTRODUCTION
Depression is a common disorder among cardiac patients, with a prevalence rate of 15%-30% [12]. It not only affects physical function, physical ability, and quality of life [34] but also has an undesired impact on medical treatment adherence, which is harmful for cardiac rehabilitation (CR) [56]. Capistrant et al. [7] showed that this psychological disorder is associated with a 69% risk of sudden death risk from coronary heart disease and a 55% risk of death from cardiovascular diseases (CVDs). The role of depressive symptoms is so outstanding in developing and stabilizing cardiac conditions [38] that 34% of patients indicate that psychological factors are the main cause of their illness [910]. In light of that finding, one of the methods that can help to reduce psychological complications is participation in a CR program [1112]. CR is recommended as one of the most important measures to take after the occurrence of a cardiac event or cardiac surgery in order to reduce complications such as depression [113]. CR entails life learning along with chronic diseases or disabling conditions, and its aim is to restore patients to their highest possible levels of physical, mental, social, and occupational capacity [14]. CR programs aim to improve patients' psychological and social states, to limit the physical and psychological effects of CVDs, to minimize sudden death or repeated heart attack, and to control the symptoms of coronary artery disease [15]. These programs can decrease patients' psychological symptoms to 50%-70% [16], but some patients do show depressive symptoms at the end of the programs. The importance of this issue lies in the fact that apart from all of the problems that arise from depression [1], the mortality rate in depressed patients after CR programs is reported to be four times greater than that in non-depressed patients [16]. Therefore, in order to recognize the factors that increase patients' depressive symptoms and to control the future complications thereof, the present study investigated the predictors of aggravated depressive symptoms at the end of a CR program.
MATERIALS AND METHODS
Design and procedure
The design of the study was retrospective. The administrative data were obtained from the CR center of Imam Ali Hospital, located in Kermanshah city, Iran. The database of this government specialist heart center comprises information about cardiac patients, particularly, any history of coronary artery bypass graft surgery (CABG), percutaneous coronary intervention (PCI), myocardial infarction (MI), and valvular heart diseases (VHD) that is recorded in the CR program after the cardiac event occurs. The patients' demographic information, including type of cardiac condition, treatment method, and any comorbid conditions are recorded in the database. The registration forms are designed by heart and health specialists and experts under the supervision of the Kermanshah University of Medical Sciences, and the university's inspection unit assesses the accuracy of the data annually. In the present study, these variables were used to identify patients who were likely to show aggravated depression at the end of the CR program. Moreover, in order to evaluate the patients' psychological states, such as anxiety and depression, the Beck Depression Inventory (BDI) was administered at the beginning and the end of the CR program at this center; the hospital's outpatient CR program entailed at least 3 sessions of exercise per week for 8 weeks. For illiterate patients, the questionnaire was administered orally by the clinical psychologist of the CR ward, and their responses were recorded. After administering the BDI post-intervention and having patients orally confirm their increased rates of depression at the end of the CR program, the relevant information was recorded as yes or no. Patients who were not depressed (those who recorded scores of 1 to 4 in the primary evaluation) were excluded from the study. Meanwhile, it should be noted that this study received ethical approval from the university's ethics committee.
Participants
We identified 1,350 patients who were documented as having participated in the CR program during the 10 years between January 2000 and January 2010. Although all patient data were entered into analysis, data on some items for some patients between 2000 and 2005 were missing, which caused the SPSS ver. 21.0 for Windows (IBM SPSS, Armonk, NY, USA) software to exclude 732 patients. In addition, one patient who was identified as having high depression at the final evaluation was excluding for having earned a score less than 4, and two more patients were excluded because there was no oral confirmation of their depression scores at the end of the CR course. Ultimately, the sample size was 615 persons.
Instrument
The Beck Depression Inventory
This questionnaire was designed by Beck in 1961. It is a 21-item scale with a choice of 3 ratings for each item; thus, the score can range from 0 to 63. The results are interpreted as follows: 0-4 means possible denial; 5 to 9 reflects very mild depression; 10 to 18 reflects mild to moderate depression; 19 to 29 indicates moderate to severe depression; and 30 or higher reflects severe depression. Beck et al. [17] found the credential retest index in a oneweek interval to be 0.93.
Statistical analysis
The characteristics of the patients who completed the CR program with increased levels of depression were compared with those with decreased depression using the chi-square test for nominal and stratified variables and one-way analysis of variance (ANOVA) for continuous variables. The percentages related to distinct variables and the means and standard deviations of the continuous variables are also reported. Moreover, binary logistic regression analysis was used to determine any sociodemographic or clinical correlations with increased depression levels at the end of the CR program. Gender, age, education, marital status, treatment with CABG or PCI, diagnosis of MI or VHD, risk factors of ischemic heart disease (diabetes, hypertension, hyperlipidemia, obesity), and history of smoking were all entered into the analysis. After adjustment for gender, age, and preintervention depression score, a p-value of less than 0.05 was considered statistically significant.
RESULTS
From the total of 615 patients (488 male and 127 female) who participated in the CR program and were entered into the analyses, 66 (10.7%) completed the program with increased depression levels; the remaining 549 (89.3%) showed decreased levels (Fig. 1). Table 1 displays the patients' pre- and post-intervention BDI scores and indicates that the CR significantly reduced depression among the total population. However, there was a significant difference between pre- and post-program depression scores among the patients who completed the course with higher scores. This finding suggests that the increased depression levels were not random but were likely affected by certain sociodemographic and clinical variables.
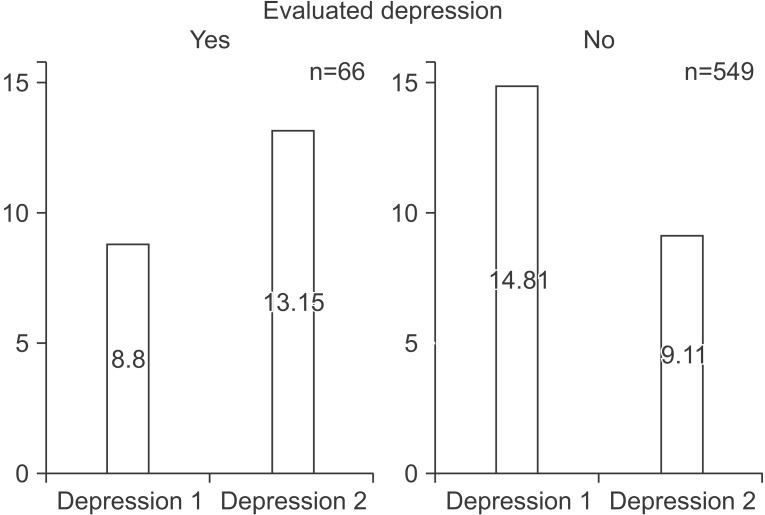
Comparison of the study participants' depression scores.

Pre- and post-intervention depression scores
The sociodemographic and clinical characteristics of the study sample are shown in Table 2. At the baseline, there were differences between the patients with and without depression in terms of education, occupation, and smoking status. Those with less education and those who were self-employed were significantly more likely to complete the CR program with increased levels of depression compared with the better educated and non-self-employed (p<0.05). With regard to the clinical variables, patients who had quit smoking were less likely to complete the CR program with increased depression levels than were those who had not quit (p<0.05).
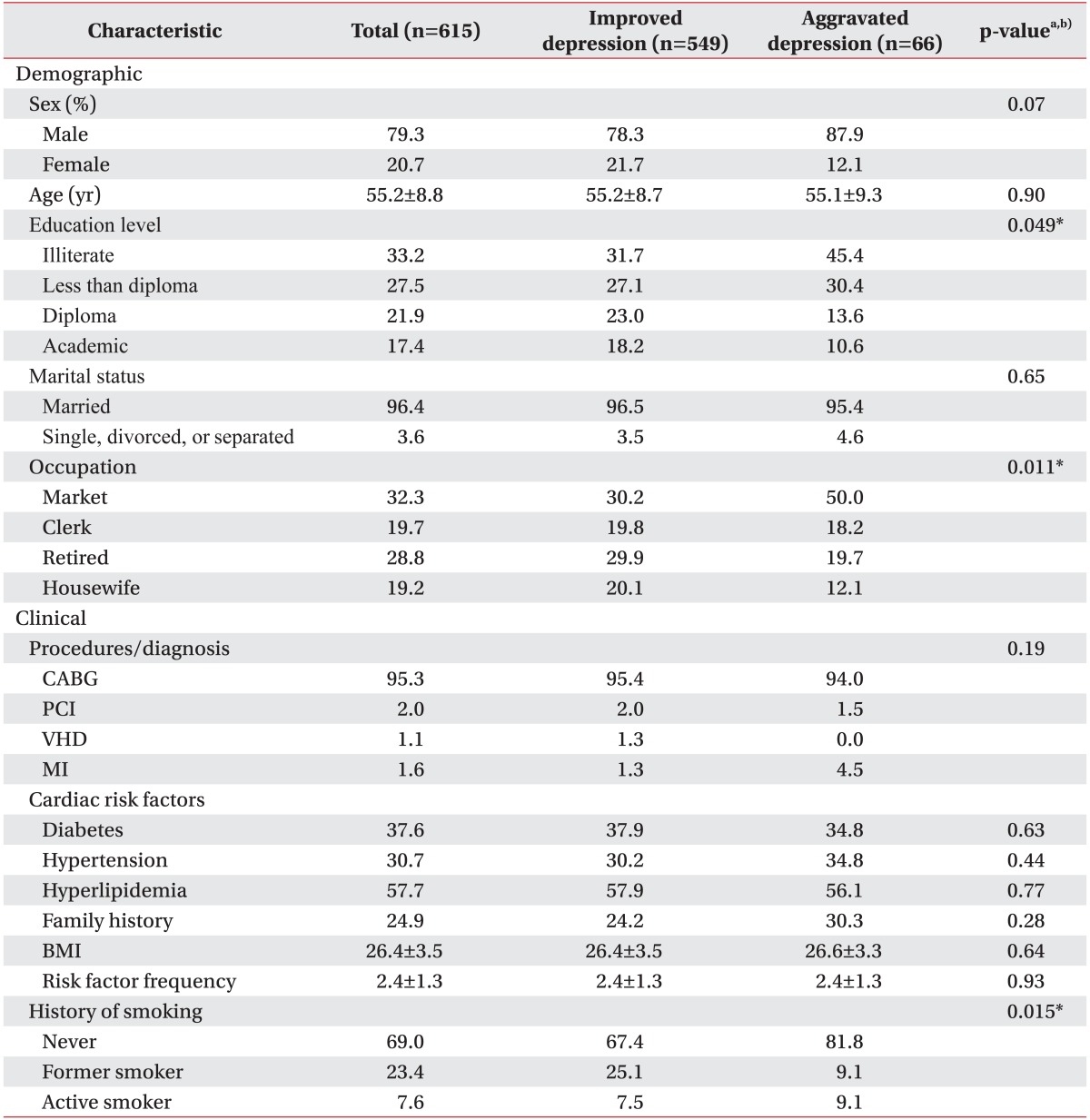
Baseline demographic and clinical characteristics in the overall population and by post-intervention depression level
Table 3 displays the adjusted odds ratio (AOR), 95% confidence interval (CI), and p-value for each covariate that was included in the binary logistic regression model. The statistical assumptions needed for a valid binary logistic regression were met, and the model was statistically significant overall (χ2=39.812, p=0.008). Of the 24 variables that were included as covariates in the regression, 3 were found to be independently significantly associated with increased depression. Indicators of effect size showed only small explanatory power with respect to increased depression (Cox & Snell R2=0.063; Nagelkerke R2=0.127). Considering the significant differences in preintervention BDI scores between patients who left the program with increased vs. decreased depression levels (F(1, 613)=38.443, p<0.0005), gender and age as well as the effect of the pre-intervention scores were controlled for. After adjustment for gender, age, and pre-intervention depression score, the table shows that the individuals who had a high school diploma (AOR=2.90; 95% CI, 1.16-7.22; p=0.022) or who had attended college (AOR=2.92; 95% CI, 1.01-8.44; p=0.047) and those who had quit smoking (AOR=4.32; 95% CI, 1.41-13.25; p=0.01) were less likely to complete the CR program with high rates of depression compared with other patients.

Predictors of increased depression in the overall population
DISCUSSION
The present study was conducted to investigate the predictors of depressive symptom aggravation among patients at the end of a cardiac rehabilitation program. The results indicate that low education level and smoking were significantly related to increased levels of depression at the end of the program. It is predicted that participating in CR programs can possibly minimize psychological symptoms such as anxiety and depression in cardiac patients in the short term; thus, it is recommended that additional studies be conducted to explore the associations [9]. The present study found that not only had some patients' depressive symptoms not decreased at the end of the program but that they had in fact increased. In agreement with Ghasemzadeh et al. [18], one of the factors in higher depression levels is a lower education level. Based on the cumulative advantage theory in health, people with higher levels of education enjoy greater health resources (such as greater capacity to avoid acute stress factors and live healthier lifestyles). Each of these beneficial resources can have a cumulative positive impact on individual health [19]. More treatment cooperation [56], desired physical functioning and higher life quality [34], and cardiac symptom control [15] could be cited as positive effects of CR programs, particularly when patients show constant and active participation in the programs [12]. Illiterate patients have more trouble understanding the guidelines, and in many cases, they are unable to appropriately implement their treatment recommendations compared with patients with higher levels of education. Although it seems that an educated family attendant could solve many of these problems, limitations such as the shortage of training and practice areas make this an impractical and unlikely solution for patients.
Another characteristic of patients with low literacy was that they felt less perceived control over their diseases compared with patients who had completed high school or any higher levels of education. Perceived behavior control is related to depression among patients with heart problems, and it independently predicted mobility, physical fitness, and regular exercise among outpatients [20]. In other words, the less the perceived behavior control, the greater the likelihood that depression severity will increase [21]. Therefore, it could be concluded that low literacy first negatively affects patients' perceived behavior control, which is then followed by severe depressive symptoms. The results suggest that patients with higher levels of education are less affected by depressive symptoms because of their greater perceived behavior control.
Other data from this study showed that patients who had quit smoking were less likely to show increased levels of depression at the end of the program compared with those who actively continued to smoke. The results of one study [22] found a significant relationship between smoking and psychological disorders and also found that anxiety along with depression are the most common comorbid conditions of smoking. Based on cognitive inconsistency theory, individuals who have multiple thoughts that cannot all be true at the same time experience tension and disorientation [23]. From a more detailed standpoint, cardiac patients who, despite the recommendations of the CR team and with their own knowledge of the increasing dangers and effects of smoking, still smoke actively will suffer from a cognitive inconsistency between their thoughts and their actions that can ultimately lead to increased anxiety and stress at the end of a CR program. This pressure increases along with progress in the CR program, and the individual becomes helpless when he or she cannot resolve the existing conflict. Regarding the relationship between helplessness and depressive symptoms [2425], increased depression levels at the end of a program would not be unlikely.
One of the limitations of this study was that the administrative data were gathered from only one hospital in western Iran, and another was the missing data that triggered the statistical software to exclude a large portion of the patients from the analyses. This missing data might have affected the generalizability of the results. Another limitation was the low number of female participants in the study. Overall, it is recommended that future studies investigate patients all around the country and also that more women be studied. Two more limitations were the retrospective nature of the data and the fact that we were not able to control for all possible confounding variables. Therefore, the impact of confounding variables must be controlled for in future studies. Finally, the present study introduced a small R square for its regression model that could have resulted from the variables that were included in the analyses, which could have resulted in incorrect predictions. It is suggested that other variables be analyzed in future studies.
Notes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.