INTRODUCTION
Endogenous, exogenous, and complex mechanisms have been presented as etiologic factors for shoulder impingement syndrome. According to Ogata and Unthoff,1 the endogenous mechanism starts with aging, circulatory disease, and differences in tensile stress within the rotator cuffmuscles, causing degenerative change and damage to the tendon of the supraspinatus muscle. They also stated that damage of the rotator cuffmuscles is due to degenerative changes in the tendon rather than by any collision and that it has no correlation with a degenerative change in the acromion.
Neer2 hypothesised that the exogenous mechanism involves the rotator cuff muscles, subacromial bursa and the long head of the biceps brachii muscle colliding with the anterior portion of the acromion and the related coracoacromial arch; this results in a disorder of the normal sliding function, causing continuous trauma every time the arm is raised and a progression to subacromial bursitis, biceps syndesmitis, and eventually inflammation and even rupture of the rotator cuff muscles.
In short, the exogenous mechanism of this thesis supports the theory that the shape of the acromion, the subacromial space, and the gradient of the acromion are correlated with damage to the rotator cuff muscles.
Also, Schamberger3 states that when the spine is bent laterally, the concave side of an intercostal space is narrowed, and this causes a depression of the shoulder joint and the scapula on the concave side. If the thoracic curvature bulges to the left, the right scapula is shown to be in retraction, depression, and downward rotation, and the facet of the glenoid fossa faces the posteroinferior side. When the slope of the glenoid shelf faces downwards, the passive support for the humerus is weakened, the capsule and rotator cuff muscles receive a great deal of traction force due to gravity, and this could be an etiologic factor in the development of supraspinatus tendinitis and other stages of the shoulder impingement syndrome.
On the basis of this study, we can therefore predict that a depression of the shoulder to the right by continuous sidewise curving of the spine may cause shoulder impingement syndrome in the right shoulder. Generally, if one compares the height of both shoulders in the standing position, most people have slight differences in the shoulder gradient. We therefore decided to investigate the relationships between the prevalence of shoulder impingement syndrome, shoulder gradient, acromiohumeral interval and location of the scapula.
MATERIALS AND METHODS
Subjects
The subjects were selected during the period April - November, 2009, from those attending the Department of Rehabilitation Medicine, who complained of pain in the shoulder and upper extremities and were diagnosed as suffering from unilateral shoulder impingement syndrome on the basis of their history and a physical examination. Patients, who were experiencing pain in the shoulder and upper extremities through trauma, fracture, bone deformities, calcification, or shoulder joint instabilities, were excluded. All patients with a restriction in their range of motion during passive joint movement were also excluded. The patients selected as candidates for this study were those, who had positive results in all three of the following physical examinations: 1) the positive painful arc sign, which causes pain at a certain angle during flexion and abduction of the shoulder joint and then loss of the pain when the angle is increased, 2) the Neer and Hawkins-Kennedy tests, 3) pain induced in the resisted isometric external rotation, abduction and elbow extension test or pain in the Jobe test. A thorough examination of the contralateral shoulder was performed to rule out any patients with bilateral shoulder impingement syndrome.
Patients diagnosed with unilateral shoulder impingement syndrome, who had rheumatism, a systemic inflammatory disease, peripheral neuropathy, a history of stroke, prior surgery in the shoulder joint or cervical vertebrae, pain in the cervical vertebrae or restriction in the movement of the cervicothoracic vertebrae, spinal disease such as scoliosis, or adhesive capsulitis, were also rejected as study participants.
Methods
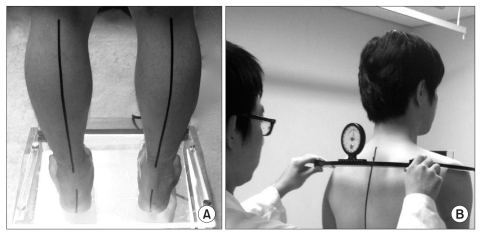
The following measurements were made on each of the 21 patients finally selected as study subjects. The shoulder gradients were obtained by having each subject stand on an angulometer with feet spread 10cm apart between both of the medial malleoli, and their heels were placed in a straight line. The ankles were fixed in a neutral position, and the knees completely extended. The relative heights of the shoulders were assessed by measuring the difference between the angles formed by both blades of the angulometer being placed on the upper, lateral side of the acromion of each shoulder (Fig. 1).
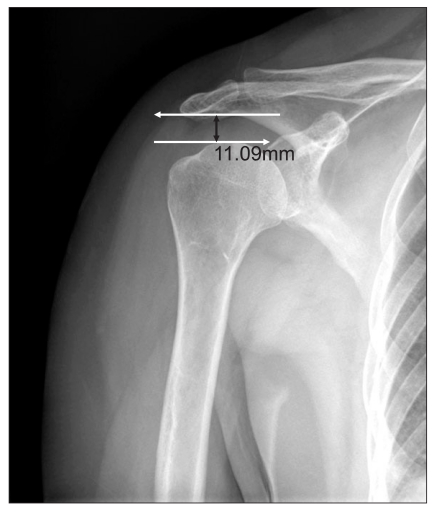
The acromiohumeral intervals were obtained from anteroposterior radiographs of both shoulders (Fig. 2). The rotation of the scapula was also obtained from the radiographs and involved measuring the angle formed by the vertical line and the line connecting the superior angle and the inferior angle. The angle was given a positive value if the scapula was rotated upwards (Fig. 3-A) and a negative value if the scapula was rotated downwards (Fig. 3-B). The average of three measurements was used.
Statistical analysis
The data were analyzed with SPSS for Windows (version 13.0). Differences between higher and lower shoulders and between shoulders affected or unaffected by impingement were compared in terms of acromiohumeral intervals and angles of scapular rotation using paired t-tests. Statistical significance was defined as a p-value≤0.05.
RESULTS
Subject characteristics
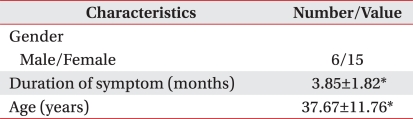
The 21 subjects (6 males and 15 females) were all right-handed, and their average age was 37.7 years (Table 1).
Prevalence of shoulder impingement syndrome in relation to the shoulder gradient
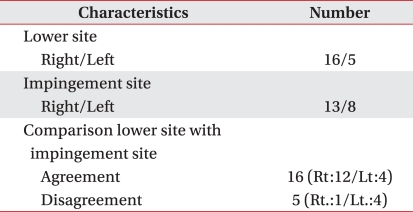
Thirteen subjects were affected with shoulder impingement syndrome in the right shoulder, and eight subjects were affected in the left. Whereas 16 subjects were affected in the relatively lower level shoulder, only five people were affected in the relatively higher level shoulder (Table 2). This observed relationship between the prevalence of impingement syndrome and the relative height of the affected shoulder was statistically significant (Fisher's exact probability test, p<0.05).
Relationship between the acromiohumeral interval and shoulder gradient
While the mean acromiohumeral interval in the relatively lower shoulder was 10.03±1.28 mm, the mean in the relatively higher shoulder was 10.46±1.50 mm, but the difference was not statistically significant. Similarly, while the mean Acromiohumeral interval of the affected shoulder was 9.98±1.29 mm, the Acromiohumeral interval of the unaffected shoulder was 10.51±1.48 mm, but again this difference failed to reach statistical significance (Table 3).
Rotation of the scapula and shoulder gradient
The mean rotational angle of -0.31±3.73 degrees in the relatively lower shoulder was significantly less (p<0.05) than the mean of 3.85±4.42 degrees in the relatively higher shoulder. Also, the shoulders affected by impingement syndrome had a mean angle of 0.00±3.72 degrees, which was significantly less (p<0.05) than the mean angle of unaffected shoulders (3.54±4.71 degrees) (Table 4).
DISCUSSION
This study determined the relationships between the shoulder gradient and the site and prevalence of shoulder impingement syndrome, the Acromiohumeral interval, and level of the scapula. The prevalence of unilateral shoulder impingement syndrome was higher in the relatively lower level shoulder, and the scapula of the lower shoulder was significantly rotated downwards compared with the contralateral one. However, the relative levels of the right and left shoulders were not significantly associated with subscapular distance.
Schamberger3 stated that, when the spine is laterally bent, the concave side of the intercostal space is narrowed, and the scapula of the concave side undergoes retraction, depression, and downward rotation. This results in the facet of the glenoid fossa facing posteroinferiorly and the slope of the glenoid shelf pointing downwards. The passive support of the humerus is weakened, the capsule and rotator cuff muscles receive considerable traction force due to gravity, and the consequence may be supraspinatus tendinitis or shoulder impingement syndrome. The theory that continually bending the spine sideways, which lowers the shoulder to the right, could cause shoulder impingement syndrome in the right shoulder joint was supported in the present study by the higher frequency of shoulder impingement syndrome in the relatively lower shoulder when both shoulder levels were compared in unilaterally affected patients. Likewise in our study, the scapula of the lower shoulder was relatively rotated downward.
A shortening of the Acromiohumeral interval, which provides the space for movements of the rotator cuff muscles, will probably increase the risk of damage to the rotator cuff muscles. Radiologic studies have shown that supraspinatus rupture occurs if the Acromiohumeral in terval is 6 mm or less, and that associated multiple muscle ruptures are highly likely if the distance is 7 mm or less.12 Park et al.13 reported that the Acromiohumeral interval measured using MRI was significantly reduced in the affected shoulder (7.7 mm) compared with that in the normal unaffected shoulder (10.3 mm). However, in our study, there was no statistical difference between the measurements of the Acromiohumeral interval in the affected (9.98±1.29 mm) and unaffected (10.51±1.48 mm) shoulders even though the Acromiohumeral interval of the affected shoulder was shorter compared with the unaffected side. This is probably due to our recruitment of comparatively young subjects with a mean age of 37.7 years and their short histories of shoulder impingement syndrome.
Shiri et al.17 found that there was a higher prevalence of biceps tendinitis and rotator cuff damage related to shoulder impingement syndrome in the dominant arm. In our study, 13 patients out of 21 patients, who were all right handed contracted shoulder impingement syndrome on the right side, but the difference was not quite as large as in the study by Shiri et al. However, 16 subjects of the 21 right handed patients were observed to have lower shoulder levels on the dominant side. Nevertheless, since our study did not include any left-dominant subjects, further studies are needed to investigate an association between shoulder gradient and the dominant hand.
The limitations of this study include the small sample size and a lack of evaluation of three-dimensional movements in the tilting or transverse rotation of the scapula. In addition, there is the need in future studies to take into account the many variables, which might cause differences in shoulder levels, such as the different lengths of the lower extremities and the level of the pelvic bone. Nevertheless, the findings of the present study suggest that an effective treatment for shoulder impingement syndrome may be found by correcting the factors responsible forincreasing shoulder gradients. Future studies should be directed towards evaluating the effectiveness of this approach.