INTRODUCTION
Spinal cord injury without radiologic abnormality (SCIWORA) was first introduced by Pang and Wilberger in 1982 [1]. SCIWORA diagnostically refers to a specific type of spine cord injury without abnormalities discovered seen in both plain radiography and computed tomography (CT), while clinically manifesting acute traumatic myelopathy, mostly involving the cervical spinal cord.
However, magnetic resonance imaging (MRI) is preferred to CT in radiologically diagnosing spinal cord injury because of its higher soft tissue contrast resolution than CT. Moreover, the resolution of MRI has been developed significantly since the diagnostic criteria for SCIWORA was previously documented [2].
Thus, the scope of SCIWORA has been narrowed nowadays, and spinal cord injuries without abnormal MRI findings are extremely rare [2,3].
We introduce an atypical case of tetraplegic spinal cord injury with normal MRI findings in every segment of the spinal cord and intact urodynamic functional, though he showed profound limb paralysis and absent somatosensory evoked potentials (SEPs) from the lower limbs.
CASE REPORT
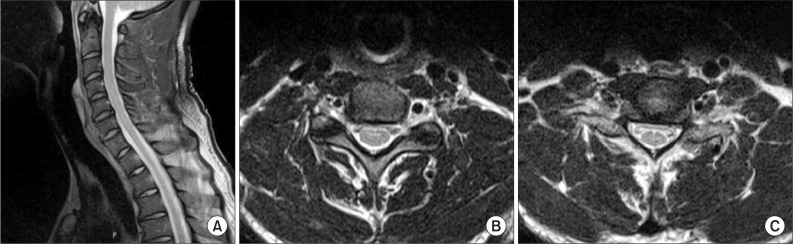
A 42-year-old male had no relevant disease history and was transferred to our department on February 7, 2014 for rehabilitative treatment for injuries sustained in a traffic accident on October 14, 2013. As a result of the accident, he underwent cervical MRI and a brain CT, which confirmed that he did not have significant abnormalities, other than slightly herniated cervical and lumbar discs (Fig. 1). During the initial physical examination, we performed manual muscle testing (MMT) according to accepted standards. The key muscle strength from C5 to C8 was of grade 4/5, the strength of the finger abductors (T1) was of grade 1/5, and the lower extremity strength (L2-S1) was of grade 2/5. He felt hypoesthesia below the C3 dermatome level, and there was no abnormality in anal sensation. The neurological level was of C3 with an ASIA grade of C. He complained of neuropathic pain equivalent to grade 4 in the visual analogue scale and presented no pathologic reflexes, such as Hoffman sign, or ankle clonus. The patient also had no clinical manifestation of neurogenic bladder and bowel symptoms, which was atypical. During MMT after 2 weeks, the patient presented improvement in the finger abductors to grade 2/5, but no other physically significant changes were observed.
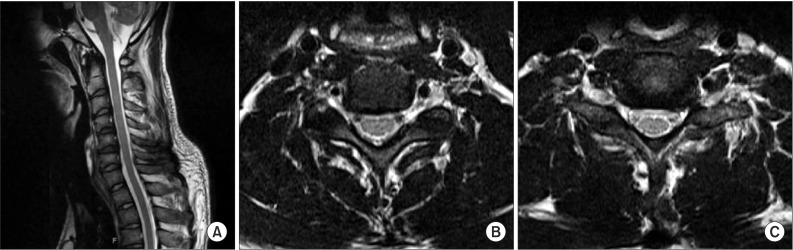
The MRI performed when the patient was transferred to our department showed no significant difference when compared to the previous imaging (Fig. 2). The results of the urodynamic study were normal, and no abnormalities were found from the intravenous pyelography and cystourethrography. No abnormalities were observed during electromyography, inclusive of motor and sensory nerve conduction tests, and bulbocavernosus reflex latency tests, save for right lumbosacral radiculopathy. However, the fact that no SEP was observed when testing both the tibial and the peroneal nerves and the extant results from the physical examination indicated that the patient suffered from an atypical traumatic spinal cord injury.
DISCUSSION
According to Pang and Wilberger [1], SCIWORA can be categorized into four groups according to age. Those from group 3 feature a radiological abnormality in the vertebral body or joints when they develop a spinal cord injury, barely manifesting SCIWORA. The pathophysiology of SCIWORA is known to manifest when an apparent radiological normality is observed due to minimal tissue damage due to stretched muscles and reflexive rigidity due to spinal hyperextension in response to a spinal cord injury [1].
According a case report presented by Kothari et al. [4], an MRI is the most accurate way to determine the mechanism for SCIWORA. This case study looked at four SCIWORA adult patients who were examined for spinal abnormalities as well as the diagnostic value of the MRI. According to Boese and Lechler [3], only 7% of SCIWORA patients were free from abnormalities based on MRI results. Furthermore, a study by Tewari et al. [2] found that four out of 40 (10%) SCIWORA patients were free from abnormalities based on MRI results.
According to the large majority of case reports on SCIWORA patients, typical tetraplegia is accompanied by urodynamic or neurological abnormalities, and pathologic reflexes are also usually impaired in most cases. According to the case report presented by Van Buul and Oner [5], an adult paraplegic patient with thoracic SCIWORA also presented with abnormal pathologic reflexes. Despite there being no specific findings upon an initial MRI, an abnormality was observed in a subsequent MRI performed two days later. Furthermore, according to a case report presented by Lee et al. [6], a delayed tetraplegic patient with cervical SCIWORA was concomitantly diagnosed neurogenic bladder and bowel symptoms, and had abnormal deep tendon and pathologic reflexes. This was a trend that was observed in the majority of cases of tetraplegic patients, with relevant abnormalities observed upon a subsequent MRI.
In our case, the patient has no apparent abnormalities in terms of a spinal cord injury, urodynamic function, and pathologic reflexes based on MRI. However, we did find abnormalities during the physical examination and the SEP test, indicating the manifestation of atypical traumatic tetraplegia. According to Sharma et al. [7], adults rarely contract SCIWORA relative to infants and constitute a mere 12.4% of the entire SCIWORA patient population, and the foregoing percentage varied by up to 10% under the research conducted by Tewari et al. [2]. A mere 10% of them were observed to have no radiological abnormalities in the spinal cord under plain radiography, CT, and MRI.
The present case manifested adult SCIWORA, including MRI, which is the first-of-its-kind to be domestically reported by anyone. There were no special findings during the MRI and the urodynamic study, and the spinal cord injury was confirmed during the physical examination and the SEP test [1,2,7]. Most spinal cord injuries are diagnosed by performing a radiological study, including MRI. However, when the diagnosis cannot be made through MRI, physical examination and a SEP test should be used to determine the presence of SCI. In this case, atypical tetraplegia was present with no radiological and urodynamic abnormalities. However, the SEP test confirmed the spinal cord injury, and the results are in agreement with the research conducted by Pang [8], who stated that the SEP test was useful in the diagnosis of SCIWORA. In this sense, the SEP test must be conducted in addition to a conventional physical examination and a urodynamic study to diagnose an atypical adult tetraplegic patient with no other abnormalities observed during radiological study, including MRI.