The Differences in Clinical Aspect Between Specific Language Impairment and Global Developmental Delay
Article information
Abstract
Objective
To compare and analyze the clinical characteristics of children with delayed language acquisition due to two different diagnoses, which were specific language impairment (SLI, a primarily delayed language development) and global developmental delay (GDD, a language delay related to cognitive impairment).
Methods
Among 1,598 children who had visited the developmental delay clinic from March 2005 to February 2011, 467 children who were diagnosed with GDD and 183 children who were diagnosed with SLI were included in this study. All children were questioned about past, family, and developmental history, and their language competences and cognitive function were assessed. Some children got electroencephalography (EEG), in case of need.
Results
The presence of the perinatal risk factors showed no difference in two groups. In the children with GDD, they had more delayed acquisition of independent walking and more frequent EEG abnormalities compared with the children with SLI (p<0.01). The positive family history of delayed language development was more prevalent in children with SLI (p<0.01). In areas of language ability, the quotient of receptive language and expressive language did not show any meaningful statistical differences between the two groups. Analyzing in each group, the receptive language quotient was higher than expressive language quotient in both group (p<0.01). In the GDD group, the Bayley Scales of Infant Development II (BSID-II) showed a marked low mental and motor quotient while the Wechsler Intelligence Scale showed low verbal and nonverbal IQ. In the SLI group, the BSID-II and Wechsler Intelligence Scale showed low scores in mental area and verbal IQ but sparing motor area and nonverbal IQ.
Conclusion
The linguistic profiles of children with language delay could not differentiate between SLI and GDD. The clinicians needed to be aware of these developmental issues, and history taking and clinical evaluation, including cognitive assessment, could be helpful to diagnose adequately and set the treatment plan for each child.
INTRODUCTION
Neurodevelopmental disorders mean any abnormalities in gross motor, fine motor, language, cognition, emotion, and personal-social areas [1]. With changes in socio-economic environments, the birth rate was declining and the average maternal age at first childbirth was rising. Late childbearing increases the risks of premature birth and low birth weights, which increase the number of children with neurodevelopmental disorders [2,3].
In Korea, there were not many studies on the prevalence of neurodevelopmental disorders, but, in the United States, it has been reported that 5% to 10% of preschool children showed developmental problems [4]. In particular, the delayed language development and communication disorders were reported to comprise the highest percentage, with 3% to 20% [5,6,7] of neurodevelopmental disorders. According to another report, language delay was the chief complaint of 41% of children who visited developmental delay clinics [8].
One of the unique characteristics of the neurodevelopmental disorders was that there were many cases that showed the overlapping and complex problems that came from many developmental areas. The language and cognitive assessments were conducted on children whose chief complaint was language delay and showed lower indexes in motor development, cognitive, and social function [4]. Another study reported that in about 34% of children who visited a hospital because of lagging behind peers in language ability, one or more delays were observed in other areas, including speech [5]. In brief, many studies have reported that in children who visited hospitals due to language delay as their chief complaint, problems were observed in other areas, not to mention the language area.
Early diagnosis and treatment was crucial to minimize the developmental delays, restore normal developmental function, and maximize ability [6,7]. In order to design an individualized management plan for each child with a neurodevelopmental disorder, an accurate diagnostic categorization should be made early. A child diagnosed with specific language impairment (SLI) will not have the same therapeutic strategy as a child who has been diagnosed with global developmental delay (GDD) [9]. The prognosis was poorer in children with GDD than in those with SLI.
However, it was very difficult to distinguish children with SLI and GDD only on the basis of a chief complaint, such as delayed language development, in an outpatient clinic. In this study, the two groups were compared in terms of history, clinical aspect, and assessment results in order to find out factors that can identify their respective characteristics and differentiate one from the other.
MATERIALS AND METHODS
Subjects
This study was conducted on 467 children diagnosed with GDD and 183 children with SLI out of 1,598 children who visited the Developmental Delay Clinic of National Health Insurance Service Ilsan Hospital from March 2005 to February 2011. GDD referred to the symptom complex in the young child, where there was a delay in skill acquisition in two or more developmental domains, with 'significant' meaning performance 2 or more standard deviations below the mean on objective norm-referenced standardized tests. The tests the children took were the Peabody Developmental Motor Scale second edition (PDMS-2), Sequenced Language Scale for Infants (SELSI) or Preschool Receptive-Expressive Language Scale (PRES), Bayley Scales of Infant Development II (BSID-II) or Korean version of Wechsler Preschool and Primary Scale of Intelligence (K-WPPSI), or Korean version of Wechsler Intelligence Scale for Children III (K-WISC-III) and Childhood Autism Rating Scale (CARS). For instance, the index score of BSID-II showed less than 50 and the total language performance was below 1 percentile in PRES, resulting in the child being diagnosed as GDD [10].
SLI was confined to cases where expressive communication or receptive language was lagging behind the peer group average without intellectual, hearing, and neurologic deficits [8,11].
If the children was diagnosed with GDD or SLI according to the definition and he or she also had a diagnosis of cerebral palsy, autism spectrum disorders, the sequelae of acquired brain lesions, or the hearing impairment, then they were excluded.
Methods
A questionnaire survey was conducted on all the children, through which information was obtained on the histories of their birth, development, their mothers' pregnancy, and their families. The children were examined by doctors of rehabilitation medicine and pediatric neurology and psychiatry, and all had the speech and language and full cognitive assessments. Some had brain MRI, and electroencephalography (EEG) was undertaken on the children who had histories of nonfebrile seizure or suspicious epilepsy.
Past history
A questionnaire survey was conducted to trace factors that might affect the development of children and included prenatal, natal, and postnatal factors. Prenatal factors consisted of eclampsia, threatened abortion, hydramnios or oligoamnios, placenta previa, and multiple pregnancy. Maternal factors, such as diabetes, hypertension, hyperthyroidism, chorioamnionitis, premature rupture of membranes, smoking or drinking during pregnancy, drugs taking history during pregnancy, depression, and anxiety, were also included for prenatal factors. For natal risk factors, premature birth, low birth weight, asphyxia, cerebral hemorrhage, jaundice, infection, and meconium staining were investigated. In postnatal factors, neonatal convulsion, sucking difficulty, and sleep disorders during neonatal period were subjected to the analysis.
The developmental history was assessed in relation to motor and language development. An inquiry was made into motor development by use of the developmental milestones. The parents were consistent in remembering the age when their child started walking on their own. Language development was assessed based on the age when the child said his or her first word.
In the case of family history, an inquiry was made into whether the child's parents, brothers, and sisters had language delays.
Language assessment
In consideration of their language abilities, full language assessments were included with SELSI or PRES. A child's receptive language score was divided by chronological age, which was converted into a percentage and was defined as 'receptive language quotient'. The same was applied to 'expressive language quotient' [12,13]. Such quotients were to make an inter-group comparison with respect to language developmental delay.
Cognitive assessment
Cognitive assessments were conducted with K-WPPSI and K-WISC-III. Children aged 3 or under who were too young to take those tests, instead took the BSID-II. When the Mental Developmental Index (MDI) or Psychomotor Developmental Index (PDI) was less than 50 on the test and thus lacking in discrimination, the mental development age or motor development age was divided by the child's chronological age, wherefrom a calculation was made of a mental development quotient (MQ) or psychomotor developmental quotient (MoQ) to make an intergroup comparison with respect to cognitive developmental delay.
Statistical analysis
The SPSS ver. 21.0 (IBM SPSS Inc., Armonk, NY, USA) was used for statistical analysis. Descriptive statistics were used for analysis of receptive language, expressive language, mental development, and psychomotor developmental quotient. An independent t-test was conducted to determine statistical differences of histories, language ability, and cognitive function between the two groups. The significance level was defined as the point at which the p-value was less than 0.05.
RESULTS
All the children were 52 months old on average at the time of their first examination (the youngest, 12 months; the oldest, 6 years) (Table 1). Boys were 420 out of 650 and thus accounted for 64.6%.

Demographic characteristics of GDD and SLI
Perinatal history
Prenatal problems were observed in 51 (10.9%) of GDD and 17 (9.3%) of SLI. The natal risk factors were in 87 (18.6%) of GDD and 28 (15.3%) of SLI, and the postnatal factors showed in 113 (24.2%) of GDD and 35 (19.1%) of SLI with no significant difference between the two groups. The gestational age averaged 39.3 months in children diagnosed with GDD group and 39.1 months in ones in the SLI group, and thus there was no significant intergroup difference. The birth weight averaged 3,113 g in the GDD group and 3,212 g in the SLI group, and therefore did not show significant inter-group difference. Twenty-six children (6.4%) in the GDD group were premature infants who were born before 37th week. In the SLI group, 13 children (4.6%) were premature infants. Likewise, there was no significant inter-group difference. Fifty-one children (10.9%) in the GDD group had been low-birth-weight infants less than 2,500 g and so were 7 (3.8%) in the SLI group. Again, there was no significant inter-group difference (Table 2).

General characteristics of GDD and SLI
Developmental history
Motor development was based on the age at which a child started walking on his or her own. On average, the children in the GDD group and the SLI group started walking on their own 18.4±7.2 and 13.9±2.6 months, respectively. Thus, the two groups showed a statistically significant difference (p<0.01). Language development can be assessed as the age at which a child says his or her first word. The two groups were found to say their first words 19.1±14.1 and 17.0±7.2 months, respectively, but did not show significant inter-group difference (Table 2).
Family history
In the GDD group, 9.4% of children had a family history of language delay and in the SLI group, 20.2% did. Thus, the SLI group showed a significantly higher percentage (p<0.01) (Table 2).
Electroencephalography
Two hundred forty-nine children in the GDD group had EEG, 95 (38.2%) of whom showed abnormalities, such as slow background activities or epileptiform activities. Sixty-four children in the SLI group had EEG, 5 (7.8%) of whom showed abnormalities. Thus, the two groups showed a statistically significant difference (p<0.01) (Table 2).
Language ability
In the GDD group, receptive language and expressive language quotients were 55.7 and 48.0, respectively. In the SLI group, these quotients were 66.7 and 53.9, respectively. Therefore, receptive language and expressive language quotients were lower in the GDD group than in the SLI group, but the difference was not statistically significant (Table 3).

Comparison of language ability between GDD and SLI
In children with GDD, receptive language and expressive language quotients were 55.7 and 48.0, respectively; receptive language quotient was significantly higher than expressive language quotient (p<0.01). In the children with SLI, receptive language and expressive language quotients were 66.7 and 53.9, respectively. As in the GDD group, their receptive language skill was on a significantly higher level than expressive language skill (p<0.01) (Table 3).
To know the percentage of expressive language involvement in each group, a count of the children whose receptive language age was 12 months ahead of expressive language age was made. In the GDD group, there were 19 children (6.2%) whose expressive language involvement was more predominant. There were 14 (8.1%) such children in the SLI group.
Cognitive ability
In the GDD group, the Bayley scale showed that the MQ and the MoQ were 47.1 and 50.1, respectively. In the SLI group, MQ and MoQ were 66.9 and 82.4, respectively. Altogether, the GDD group was remarkably inferior to the SLI group in MQ and MoQ (p<0.01) (Table 4). In both groups, MoQ was assessed at a slightly higher level than MQ, but a statistically significant difference was observed only in the SLI group (p<0.01) (Table 4).

Comparison of cognitive function between GDD and SLI by BSID-II
In the GDD group, the Wechsler test showed that the verbal intelligence quotient (VIQ) and the performance intelligence quotient (PIQ) were 67.5 and 62.7, respectively, and VIQ was significantly higher than PIQ (p<0.01) (Table 4). In the SLI group, VIQ averaged 79.0 and thus stood at the borderline. Performance IQ was assessed at 89.2, on a low average level. Their difference was worked out at -9.8 (±14.2), which was statistically significant (Table 5). Like the Bayley scale, the Wechsler test showed that VIQ and PIQ were all higher in the SLI group than in the GDD group (Table 4).
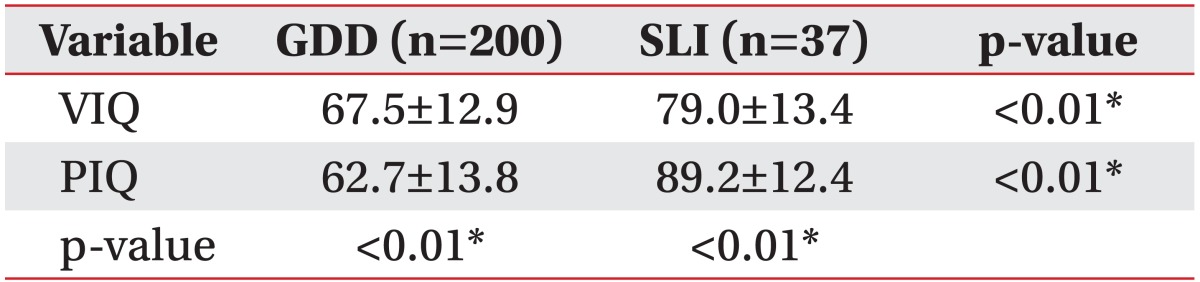
Comparison of cognitive function between GDD and SLI by K-WPPSI/K-WISC-III
DISCUSSION
Delayed development in childhood can be defined as a difficulty in achieving the same specific developmental milestones as chronological peers. Significant delay was captured by performance that was two standard deviations or more below the mean on age-appropriate, standardized, and norm-referenced testing [14]. Developmental delay can be classified to the global or single domain. GDD was evidence of significant delay in two or more of the following developmental domains: gross/fine motor, speech/language, social/personal, cognition, and activities of daily living. Typically, a delay in two developmental domains was associated with delay across all domains evaluated [15]. GDD was a distinct diagnostic entity of a young child, such as a child under 5 years of age, but in this study we involve some 6 years old children who manifested intellectual disability later. If a child's specific function lagged behind the peer group average, single domain developmental delay, such as SLI, could be an accurate diagnosis.
Speech and language delay accounted for a large majority of visitors' chief complaints [12,16], and it may be caused by not only SLI but also GDD or intellectual disability, autism spectrum disorder, or by other motor or psychomotor developmental areas. Although their chief complaints were about the same, therapeutic approaches and the prognosis should depend upon the definitive diagnosis [17]. Herein lies the reason why the underlying diseases should be identified and therapeutic plans should be based on those diseases.
Many previous studies dealt with perinatal history as principal risk factors for GDD [18], but such factors have not been studied in children with SLI. This study compared GDD and SLI in terms of birth history. However, it could not clarify the differences in perinatal history, including gestational age and birth weight between the two groups. The reason might be that the data were collected only from children who visited this hospital, and there were not many cases of premature birth and low birth weight.
With respect to the age when children said their first words, the two groups did not show significant differences. It might be because the children from both groups showed delay since early stage of language development. With respect to the age when children started walking on their own, a memorable motor milestone, there was a statistically significant inter-group difference; the GDD group was found to be significantly delayed. This snippet of information can be taken from a brief questionnaire but can be very important information to obtain an impression of more global developmental problem.
According to a study by Bishop et al. [19], among children who were consistently having language delay, their first-degree relatives were found to have a history of language delay. In addition, many studies were carried out on the correlation between language impairment and genetic factors and reported that SLI highly correlated with family history [20,21]. This finding that SLI has significant relevance to family history was consistent with this study.
Cho et al. [4] reported that a group with mixed receptive-expressive language disorder received low grades, even in motor development, cognition, and social maturity, but another group with specific expressive language impairment did not. A study by Kim et al. [17] reported that the receptive language was better than expressive language function in SLI group while that difference was not apparent in mild intellectual disability group. In this study, the SLI and GDD groups did not show obvious difference in receptive and expressive language development. When receptive language was 12 months ahead of expressive language, the authors regarded it as clinically significant, and calculated the percentage of such children in each group. Such children accounted for 6.2% of the GDD group and 8.1% of the SLI, and thus there was no significant inter-group difference. In this study, resultantly, there were no distinct inter-group differences in linguistic features, which implied that the differential diagnosis of SLI and GDD cannot be based solely on the results of language assessments.
Shevell [18] conducted a study on children with GDD and SLI when they were preschoolers and were retested through cognitive function tests after they attended elementary schools. The GDD group got very low grades in Bayley scale or Wechsler tests. SLI children had specific developmental problems in a single domain, not in the cognitive area as a whole. In GDD children, the finding of the Bayley scale showed no difference in the severity of mental and motor delay, but the Wechsler test showed PIQ was more severely involved. It was hard to say that these changes in cognitive ability were related to age. Rather, the characteristics of tests of this study should be regarded. The Bayley scale was developed to assess development and the Wechsler test was for intelligence [22]. The two test scores were not interchangeable and represented unique characteristics of each area.
This study had some limitations in relation to the generalization of results. It was because the visitors to the developmental delay clinic could be more likely to have more severe developmental delay. Apart from that, the results were expected to offer a useful predictor at the time of initial diagnosis insofar as objective data were collected from a large number of children.
In conclusion, it was standard practice to conduct language assessment on children whose chief complaint was language developmental delay, but the results of this study showed that it was difficult to distinguish GDD from SLI simply on the basis of language assessment. In this context, physicians should identify the clinical aspects, including the developmental history of motor function, the family history of language delay, and the cognitive assessment, which may allow for distinctions to be made between the two groups. In the interest of early diagnosis and effective treatment, it was crucial to implement comprehensive and wide-ranging assessment for children with language delay and then to find overlapping problems.
Notes
No potential conflict of interest relevant to this article was reported.