Dementia Epidemiology Fact Sheet 2022
Article information

Abstract
This dementia epidemiology fact sheet 2022 is aimed at providing an overview of the epidemiology of dementia in Korea using representative government-led data. This review summarizes the prevalence and incidence of this condition using various types of data. The prevalence and incidence of dementia have increased and are predicted to continue to do so. This information will be utilized by public health officials, healthcare professionals, and policymakers to develop strategies for dementia rehabilitation and prevention.
INTRODUCTION
Dementia is a syndrome characterized by the deterioration of cognitive function beyond that expected as a result of biological aging. It manifests as a disturbance of multiple higher cortical functions including learning and memory, complex attention, executive function, language, motor perception, and social cognition, which affect one’s ability to perform everyday activities independently [1]. The World Health Organization (WHO) estimates that the number of individuals with dementia worldwide is approximately 55 million, with this number expected to reach approximately 78 million by 2030 and 139 million by 2050 [2]. The global financial burden of dementia was estimated to be US$ 1.3 trillion in 2019 and may rise to US$ 2.8 trillion by 2030.
These trends seem to be more pronounced in Korea, a country experiencing rapid aging of its population; the number of people aged 65 and older reached 8.53 million in 2021 and is expected to exceed 12.98 million by 2030, and 19 million (accounting for 39.8% of the older adult population) by 2050 [3]. These projected population figures suggest that dementia will become an increasingly significant challenge. Dementia has a profound impact at both individual and societal levels, such that the estimated health-economic cost per capita for dementia in Korea was approximately US$ 6,957 in 2019 [4].
Recognizing the enormous impact of dementia in Korea, the Korean Academy of Rehabilitation Medicine launched its first “Dementia Epidemiology Fact Sheet” in 2022, with a plan to update it periodically. This fact sheet provides contemporary statistics on dementia in Korea which may contribute toward future studies and policies involving dementia rehabilitation and prevention.
The most commonly referenced epidemiological statistics are disease prevalence and disease incidence. Dementia prevalence refers to the number of people with dementia at a given point in time, whereas dementia inAnnals cidence refers to the number of new cases of dementia diagnosed over a specified time period. Here, we report on the prevalence and incidence of dementia among individuals aged 65 years and older in the Korean population. Dementia prevalence in Korea varies depending on the methods and population used in a given study [5]. Thus, we prioritized the government-led, populationbased, nationwide report. The present review, therefore, quoted (1) the Nationwide Survey on Dementia Epidemiology of Korea (NaSDEK); (2) statistics from the Ministry of Health and Welfare of Korea and the National Institute of Dementia (NID)—Korean Dementia Observatory (KDO) report and “Dementia Today” [6]; and (3) statistics from National Health Insurance Service (NHIS) claims data. As the incidence of dementia in Korea has rarely been reported, studies using government-led data were used to derive the following statistical values.
PREVALENCE
Prevalence from NaSDEK
The NaSDEK calculated national standardized dementia prevalence by adjusting crude prevalence according to age, sex, education, and region-applied sample weights, based on the national population census survey data obtained by Statistics Korea during the corresponding time period. It reported the estimated dementia population, standardized dementia, mild cognitive impairment (MCI) prevalence, and standardized dementia prevalence according to the Clinical Dementia Rating (CDR) stage. The NaSDEK also reported the estimated dementia prevalence at a specific point in time using standardized dementia prevalence at the time of publication (Table 1). The NaSDEK was compiled using data from older Korean adults who were randomly sampled from 15 administrative districts across the country [7]. The population was selected by region-based, multi-staged sample extraction, which was performed primarily in hospital settings rather than in nursing homes or nursing hospitals; therefore, the reported prevalence is likely an underestimation. Nonetheless, the methodology used in the NaSDEK was substantial enough to deem the prevalence data representative.

The NaSDEK was conducted in 2008 [8], 2012 [9], and 2016 [10], and reported the point prevalence rate of dementia, which is the prevalence of dementia at a particular point in time. While both the 2008 NaSDEK and the 2012 NaSDEK were conducted on older adults aged 65 years or older, the 2016 NaSDEK surveyed populations were aged 60 years and above. This broadening of the age criterion was done to standardize the age threshold of government-led dementia management projects. The latest survey was conducted using 5,056 participants with a two-stage design, in which the 1st stage screened for dementia using the Mini-Mental State Examination for Dementia Screening (MMSE-DS) criteria [11], and the 2nd stage diagnosed dementia using clinical criteria laid out by the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD-K) [12] and CDR [13]. A diagnosis of dementia was made according to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition [14]. For the populations diagnosed with dementia, subtyping of dementia into Alzheimer dementia (AD) and vascular dementia (VD) was performed according to the National Institute of Neurological and Communicative Disorders and Stroke, the Alzheimer’s Disease and Related Disorders Association criteria [15], and the Association Internationale pour la Recherche et l’Enseignement en Neurosciences criteria [16]. MCI was defined according to the revised consensus criteria of the International Working Group for MCI [17].
The estimated number of patients with dementia was 703,968, which accounted for 9.95% of the cases of dementia among older adults aged 65 years and older reported in the 2016 NaSDEK. Raw data at each NaSDEK demonstrated a continuous increase in dementia prevalence. However, a recent report directly compared the 2008 and 2016 NaSDEKs using identical populations, as well as structure-based age- and sex-standardizations (based on the 2015 population structure obtained from the National Statistical Office in Korea), and concluded that the prevalence of dementia had decreased, although not significantly [7].
In 2016, the prevalence rate of dementia by subtype was 7.07% for AD, 0.83% for VD, and 1.60% for other types of dementia. From 2008 to 2016, VD prevalence demonstrated a continuous decrease, while the prevalence of AD increased; as a result, the 2016 NaSDEK reported that the AD/VD ratio measured approximately 8.5:1 among older adults. This dissociating trend in prevalence between VD and AD has been reported in previous studies. Prevalence in the Japanese population demonstrated an increase in AD and no change in VD [18]. A systematic review of dementia prevalence in Korea showed that the AD/VD ratio changed from 1.96 in the early 1990s to 4.13 in the late 2010s [5]. The review also suggested that the prevalence of severe dementia has decreased, and that of milder forms of dementia has increased.
The distribution of the severity of dementia in 2016 was as follows: 48.4% had questionable dementia (CDR 0.5), 27.6% had mild dementia (CDR 1), 21.9% had moderate dementia (CDR 2), and 2.1% had severe dementia (CDR 3) [7]. Increasing proportions of mild dementia accounted for the majority of cases, suggesting that early screening for dementia and appropriate medical care are of increasing importance. On the other hand, MCI showed inconsistent trends, which might be due to more rigorous diagnostic methods for subjective cognitive decline.
Each NaSDEK reported an estimated future prevalence prediction for the reporting year. The 2008 NaSDEK predicted a dementia prevalence of 9.08%, which was close to the actual dementia prevalence of 9.18% in 2012. However, the predicted estimated prevalence increased significantly with time, with prediction values increasing to 13.17% in 2008, 15.06% in 2012, and 16.09% in 2017. This is thought to be due to an increase in the older adult population secondary to increasing life expectancy. Considering the socioeconomic costs of dementia, effective strategies and policies for diagnosis and treatment are required at the national level.
National Institute of Dementia: KDO & “Dementia Today”
The KDO report has been published annually from 2017 to 2020 by the Ministry of Health and Welfare and the NID [19-22]. Every KDO presents two different numbers of dementia patients: the estimated number of dementia patients, and the actual number of patients diagnosed with dementia. First, the estimated number of patients with dementia is calculated in a similar way to that in the latest NaSDEK. In other words, the KDO of a specific year uses the NaSDEK 2016 data and population census values for a specific year. Thus, the 2017 KDO values are similar to those of the 2016 NaSDEK. Second, the number of patients with a diagnosis of dementia is obtained from patients whose hospital medical records were confirmed by the NHIS to contain one of six disease codes (F00, F01, F02, F03, G30, G31) based on the WHO’s Global Dementia Observatory. In addition, the number of patients with MCI was obtained from patients whose medical records were confirmed by the NHIS to contain the disease code F067. Both the estimated number of dementia cases and the actual number of diagnosed patients with dementia increased continuously between the 2017 KDO and the 2020 KDO. Similarly, the prevalence of MCI has displayed a consistent increase (Table 2).

There are large differences between the 2017 KDO and the remaining KDOs as a result of differences in data sources; that is, the 2017 KDO used the severity ratio from the 2016 NaSDEK, while the other KDOs used the ratio from the 2012 NaSDEK. Thus, caution is needed when comparing trends in dementia severity from one KDO to another.
“Dementia Today” reports prevalence using data obtained from the NID website (available at https://www.nid.or.kr/info/today_list.aspx). It periodically updates the number of diagnosed patients with dementia, similar to the KDO. Therefore the latest prevalence data and the number of patients with a diagnosis of dementia are reported and are representative of the population of a given year, using the standardized dementia prevalence parameters established in the 2016 NaSDEK.
We have summarized the estimated number of dementia cases and prevalences from the NaSDEK and NID. The projected values of future figures are estimated for each report (Figs. 1, 2).
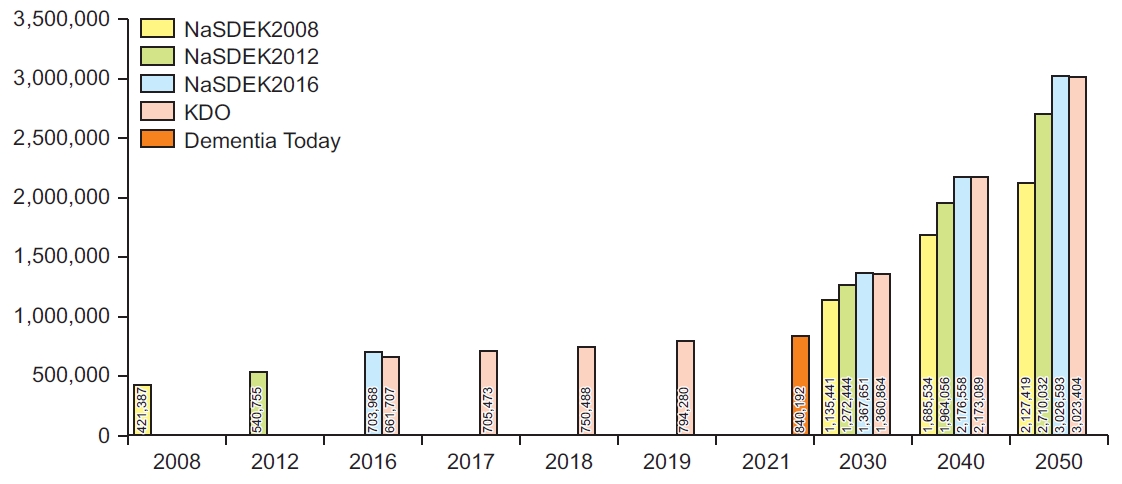
Estimated number of dementia patients in the Korean population aged 65 years and older according to the Nationwide Survey on Dementia Epidemiology of Korea (NaSDEK) and National Institute of Dementia. KDO, Korean Dementia Observatory.

Prevalence of dementia in the Korean population aged 65 years and older according to the Nationwide Survey on Dementia Epidemiology of Korea (NaSDEK) and National Institute of Dementia. KDO, Korean Dementia Observatory.
Number of people with dementia according to NHIS
The NHIS is a universal, mandatory, single-payer, nationwide health insurance system that covers approximately 100% of the Korean population [23]. As previously mentioned, collected data represents patients with a dementia diagnosis code who received inpatient or outpatient treatment. Variations with regards to diagnosis code definitions, primary, and secondary diagnoses are present.
In contrast to the data reported in the KDO and “Dementia Today,” the NHIS report [24] calculated the number of dementia patients based on the number who received a KCD diagnosis code for at least one of a multitude of dementia diagnoses: dementia in Alzheimer disease (F00, F000, F001, F002, F009), Alzheimer disease (G30, G300, G301, G308, G309), vascular dementia (F01, F010, F011, F012, F013, F018, F019), alcoholic dementia (F107), frontotemporal dementia and Pick’s disease (G3100), semantic variant primary progressive aphasia (G3101), dementia in other diseases classified elsewhere (F02), dementia in Pick’s disease (F020), dementia in Creutzfeldt-Jacob disease (F021), dementia in Huntington’s disease (F022), dementia in Parkinsonism (F023), dementia in human immunodeficiency virus disease (F024), dementia with Lewy bodies (G3182, F028), dementia in other specified disease classified elsewhere (F028), unspecified dementia (F03), and delirium superimposed on dementia (F051). It also includes codes applicable to extended health insurance claims for severe dementia: nonfluent primary progressive aphasia (G3102), logopenic primary progressive aphasia (G3103), NEC and progressive isolated aphasia (G3104).
Table 3 shows the number of patients with dementia as both the primary and secondary diagnosis. For the purpose of comparison, Table 3 contains values from other data sources in the year. The number of people diagnosed with dementia is rapidly increasing, which is thought to be due to the increasing interest in dementia by both the medical field and the general public. In comparison to the NaSDEK and KDO, the number of patients with a primary diagnosis of dementia was lower across all years. On the other hand, the number of patients who were diagnosed with dementia as the primary or secondary diagnosis was lower in 2008 and increased significantly after 2012 compared to that from the NaSEDEK and KDO data. This suggests that the actual number of patients with dementia may be much higher than previously believed, requiring a more proactive approach for diagnosing patients with subclinical or less apparent dementia.

Another method for calculating the dementia population uses injury codes applied to special cases for the Copayment Decreasing Policy: injury codes V800 (ICD codes F001, F002, F010, F011, F012, F013, G301) and V810 (F000, F020, G300, G3100, G3101, G3102, G3103, G3014, G3182) [25]. This method produced similar results to the estimated numbers obtained using cases with a primary diagnosis code of dementia (Table 3).
INCIDENCE
There are no official reports on dementia incidence from government-led data. The incidence of AD and MCI in Korea was reported in the follow-up subpopulation of the NaSDEK 2008 [8,26]. The age-standardized incidence rate of AD and MCI per 1,000 person-years was 7.9 and 28.1, respectively, among people aged 65 years and older. Recently, Jang et al. [27] reported the incidence of dementia among individuals aged 60 years and above from 2003 to 2015 using the NHIS Senior Cohort (NHISSC), which is a research database constructed in a cohort format including the 10% of the population aged 60 and above in the National Health Information Database [28]. The incidence rate per 100,000 person-years was 140.06 in 2004, 785.10 in 2008, 1,938.58 in 2012, and 2,218.25 in 2015. This rapid increase in dementia incidence might be linked to the increasing dementia prevalence in Korea, which is in contrast to the decreasing trend of dementia observed in high-income Western countries [29].
CONCLUSION
This review shows an increasing trend in both the prevalence and incidence of dementia in Korea using representative, government-led data. This updated epidemiological data will be utilized by public health officials, healthcare professionals, and policymakers to develop strategies for dementia rehabilitation and prevention. Additionally, the utilization of diverse data sources allows for a considerably broader perspective of dementia.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This research was supported by the Korean National Rehabilitation Research Institute grant (No. 22-C-03).