INTRODUCTION
Traumatic brain injury (TBI) is one of the major causes of disability. After TBI, cognitive dysfunction, behavioral changes, seizures, metabolic dysfunction, and musculoskeletal dysfunction, such as spasticity, fracture, and heterotopic ossification can occur [1]. Decompressive craniectomy (DC) is commonly performed in patients with intracranial hypertension or brain edema due to TBI. In 2016, Kramer et al. [2] performed a cohort study with TBI patients. Among 644 patients, 51 patients (about 8%) underwent DC. DC was performed when there was evidence of transtentorial herniation, worsening of midline shift, increased intracranial pressure, or loss of pupil light reflex. Complications that can arise after DC include hemorrhage, infections, and cerebrospinal fluid (CSF) disturbances [3].
After DC, cranioplasty is usually performed to improve cosmetic appearance, CSF hemodynamics, and for mechanical protection [3]. However, the optimal time between DC and cranioplasty has not been well established, and many studies have compared the efficacy of early cranioplasty (1 to 3 months after DC) with late cranioplasty (4 to 6 months after DC). One systematic review by Xu et al. [4] concluded that although early cranioplasty reduced the operation time, it increased the risk of complications. However, another systematic review by Tasiou et al. [5] concluded that early cranioplasty could lead to a better outcome.
Here, we report two cases of patients with traumatic subdural hemorrhage (t-SDH) who had neurologic deteriorations, accompanied by sunken scalp after DC. Neurologic function of both patients improved dramatically after early cranioplasty.
CASE REPORTS
This study was approved by the Institutional Review Board of the Catholic University of Korea, St. VincentŌĆÖs Hospital, and informed consents were waived after IRB approval (No. VC16ZISE0066).
Case 1
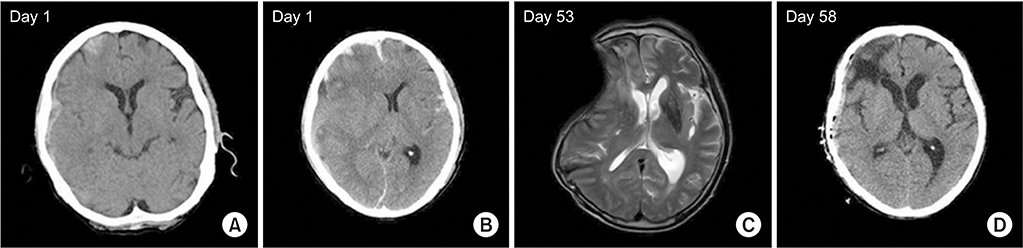
A 66-year-old male patient came to the emergency department with headache after head trauma following syncope. Brain computed tomography (CT) revealed t-SDH on the right frontotemporal lobe (Fig. 1A). A few hours later, he became drowsy and follow-up CT showed an increased amount of hemorrhage and midline shifting (Fig. 1B). DC was done that day, and motor power improved from Medical Research Council (MRC) grade 1ŌĆō2 to grade 2ŌĆō3. Seven weeks after the accident, however, he complained of shoulder pain, and his left arm weakness was aggravated to MRC grade 0ŌĆō1. Brain magnetic resonance imaging (MRI) revealed midline shifting with a sunken scalp (Fig. 1C). Early cranioplasty was done (Fig. 1D) and motor power recovered to grade 3 in a week.
Case 2
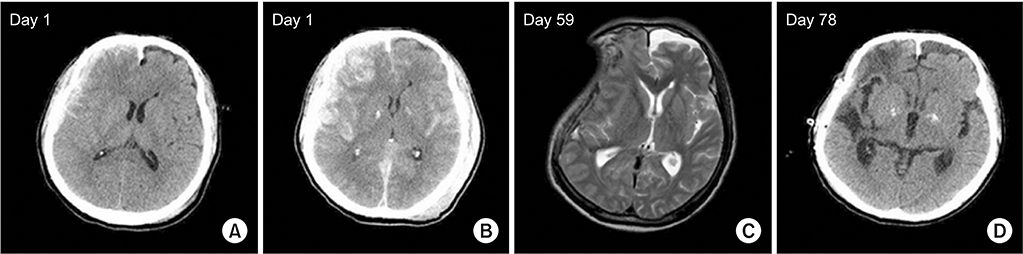
A 68-year-old male patient was hospitalized after falling from a tree. The brain CT showed t-SDH on the right frontotemporal lobe (Fig. 2A), and 4 hours later there was an increased amount of hemorrhage and midline shifting (Fig. 2B). DC was done immediately, and he showed left hemiparesis with MRC grade 3. After 7 weeks, motor power improved to MRC grade 4 on the left side, but he complained of a headache in the right temporal area. A week later, his motor power decreased to MRC grade 1ŌĆō2 on the left side. Diffusion MRI showed no acute infarction, but demonstrated midline shifting with a concave surface (Fig. 2C). Cranioplasty was performed 11 weeks after the accident (Fig. 2D), and motor power improved to MRC grade 3 on the fourth postoperative day.
DISCUSSION
Most DCs are performed in situations such as brain herniation or swelling after brain injury, and cranioplasty is performed after DC to cover the cranial defect for brain protection and for cosmetic reasons. Traditionally, surgeons prefer late cranioplasty, performed 3 to 6 months after DC, to control complications, such as swelling and infection. According to a systematic review comparing early and late cranioplasty, early cranioplasty did not show a significant advantage when compared with late cranioplasty [4]. Early cranioplasty reduced the duration of surgery, but was not effective in reducing post-cranioplasty complications, even resulting in a higher risk of hydrocephalus [4]. Salma et al. also supported delayed cranioplasty, because more bleeding complications occurred as a result of tissue fragility in patients with massive middle cerebral artery infarctions [6].
Sinking skin flap syndrome is defined as neurologic deficits with concave deformity and relaxation of the skin flap which tends to develop several weeks to months after large craniectomy [7]. In the two cases presented here, however, large cranial defects after DC resulted in a sunken scalp with neurologic deterioration. Following removal of the bone, atmospheric pressure on the cortex beneath the scalp can result in sinking skin, alterations in cerebral perfusion and flow of CSF, and neurologic deterioration, including motor weakness seen in our cases [3,8,9]. In both cases, motor weakness occurred with a sunken scalp and neurologic deterioration dramatically recovered following cranioplasty at 8 and 11 weeks after craniectomy, respectively. It is suggested, therefore, that clinicians should carefully monitor subacute TBI patients who have undergone DC.
Early cranioplasty is controversial. However, it not only has a cosmetic purpose, but a therapeutic purpose which can improve brain perfusion and CSF flow. Moreover, a recent retrospective study reported cognitive improvement after early cranioplasty [10].
When there is a rapid neurologic change in a patient with history of decompressive cranioplasty, CT should be performed first, before other less important tests. Furthermore, if a patient with sunken scalp shows any neurologic deterioration, it is important to recognize that this might be the cause of the neurologic change. Early cranioplasty should be performed when midline shifting is confirmed by CT, as in these cases, and can result in better outcomes.
Although there are published case reports [8] and studies [5,9,10] on the usefulness of early cranioplasty for sinking skin flap syndrome, we present these case reports in order to emphasize the clinical importance of management in patients with rapid neurologic change after decompressive cranioplasty. As seen in our cases, dramatic improvements of neurologic recovery are possible after cranioplasty in patients showing neurologic deficits with sunken scalp. Therefore, patients should be closely checked for neurologic deteriorations after craniectomy, and if they show ŌĆśsyndrome of the trephinedŌĆÖ, early cranioplasty should be considered.