INTRODUCTION
Osteoporosis is a global health concern with an increased in the elderly [1,2] and the treatment options include calcium, vitamin D, parathyroid hormone, strontium, and bisphosphonates [2]. The widely used bisphosphonate therapy [2], decrease bone resorption and hypercalcemia, and reduce the osteolysis of bone metastasis [1]. A number of randomized clinical trials have shown that bisphosphonates increase bone density and reduce the risk of vertebral, non-vertebral and hip fractures [2,3]. However, the possibility of severely suppressed bone turnover under long-term administration and potential long-term safety concerns such as atypical fracture or osteonecrosis of the jaw associated with bisphosphonate therapy are well reported [2-4]. Here, we present a case of bilateral femoral shaft non-traumatic stress fractures secondary to long-term alendronic acid therapy.
CASE REPORT
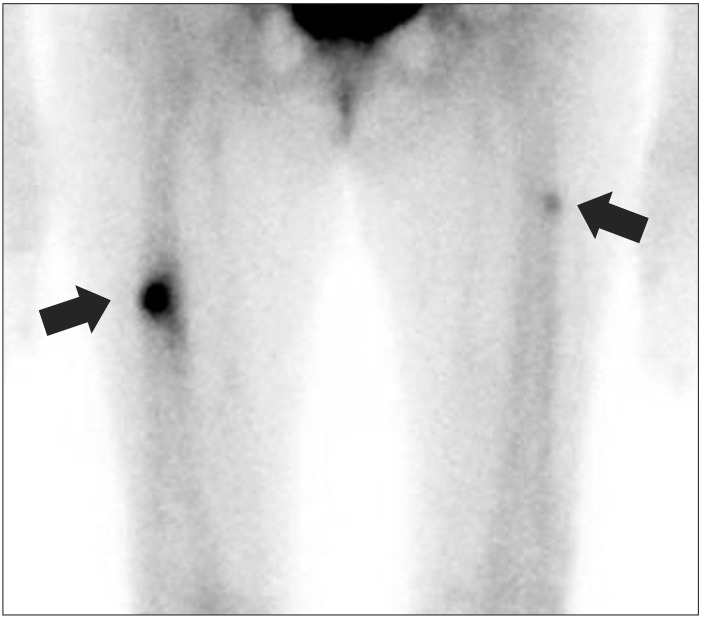
A 75-year-old postmenopausal woman presented to the rehabilitation out-patient department with a three-week history of bilateral, persistent thigh pain which was developed around the same time in both sides with more severe in right side. The patient did not have any history of trauma and her spinal stenosis was treated with decompression surgery 3 years ago. Her hypertension was treated with losartan 50 mg and hydrochlorothiazide 12.5 mg. Patient was on alendronic acid (Fosamax; MSD Korea Ltd., Seoul, Korea) 70 mg once a week for postmenopausal osteoporosis for 8 years. The most recent bone mineral density, measured by dual-energy X-ray absorptiometry showed T-scores at total lumbar vertebra of 0.2 (1.047 g/cm2), total hip of -1.5 (0.679 g/cm2), and left femur neck of -2.9 (0.496 g/cm2). On physical examination, there was a severe tenderness in bilateral mid-thigh with no swelling. The plain X-ray of right femur revealed lateral cortex thickening with transverse fracture line of mid shaft, compatible with site of pain. However, only lateral cortex thickening was shown in the plain X-ray of left femur (Fig. 1). A whole body bone scan, showed focal uptake of technetium-99m at lateral cortex of bilateral femur (Fig. 2), and an additional fracture of left side was also observed. She was referred to orthopedic surgery and underwent the open reduction and internal fixation with a plate and screws of the right femoral shaft, and with intramedullary (IM) nail and cables in the left femoral shaft. During the IM nailing in the left side, proximal bony fragment was displaced laterally, therefore, reduction using cables was required (Fig. 3). Overall, the outcome of the surgery was good without any acute complications. Alendronic acid therapy was stopped and the patient was kept under observation without any osteoporosis medication with the follow-up of bone mineral density.
DISCUSSION
The incidence of atypical fractures was estimated to be approximately 78 cases per 100,000 patients taking oral bisphosphonates [5]. These fractures have been described in patients receiving alendronate for more than 5 years [6]. Most atypical fractures occurred in patients treated with alendronate due to more frequent use of alendronate, rather than to specific pharmacological properties of this particular bisphosphonate [7].
The half-life of bisphosphonate is more than 10 years and it exerts its effects even after cessation of therapy [4]. It has been suggested that the prolonged suppression of bone turnover under long-term administration may impair the ability of bone to remodel, leading to accumulation of microdamage and compromised bone strength, ultimately progress to insufficiency stress fracture [7,8].
There are common radiographic features of atypical fractures associated with bisphosphonate use such as transverse fracture line and the appearance of beaking of the cortex on one side and bilateral thickened diaphyseal cortices [6,9].
The clinical features of these fractures are prodromal pain, typically sharp, well-localized to the mid or upper thigh, for several weeks to months prior to the fracture [7]. As described by Rizzoli et al. [9] fractures occur with minimal or no trauma and Giusti et al. [7] reported about 40% of these fracture occurred with no trauma history. Therefore, critical evaluation of patients on long-term bisphosphonate therapy presenting with pain in the thigh is required. Routine bilateral radiographs of the femur looking for stress reaction is required and if necessary, advanced imaging such as bone scan or magnetic resonance imaging should be considered.
There is no consensus for the duration bisphosphonate therapy in patient with osteoporosis. However, Black et al. [4] suggested that, for many women, discontinuation of alendronate for up to 5 years does not appear to significantly increase fracture risk compared to continuing bisphosphonate for 10 years. Also, Silverman and Christiansen [2] proposed the concept of a "drug holiday", based on evidence of sustained protection from increased bone turnover and fracture in patients who had received bisphosphonate therapy 5 or more years. Therefore, it was suggested that other options such as hormone therapy or a selective estrogen receptor modulator should be considered as an appropriate alternative for a younger population who may remain on therapy for many years [2].
In conclusion, we suggest that plain radiographs is required in patients with thigh pain and long-term bisphosphonate therapy to evaluate atypical stress fracture and discontinuation of bisphosphonate could be considered for patient with osteoporosis treated with bisphosphonates more than 5 years.