The Relationship Between Muscle Fatigue and Balance in the Elderly
Article information
Abstract
Objective
To investigate the effect of gastrocnemius muscle fatigue on postural control ability in elderly people.
Methods
Twenty-four healthy elderly people participated in this study. The postural control ability of single leg standing was evaluated with Health Improvement & Management System (HIMS) posturography before and after fatiguing exercises. After evaluating initial postural control ability, the maximal voluntary contraction (MVC) of ankle plantarflexion was assessed using a surface electromyogram from the medial belly of the gastrocnemius muscle. After a 5-minute resting period, subjects began submaximal isometric ankle plantarflexion (40% MVC) until 40% of MVC was dropped below 95% for 5 seconds, or subject couldn't continue working out due to muscle fatigue. And postural control ability was assessed after fatiguing exercise. The mean deviation of center of pressure (COP), length of COP movement, occupied area of COP were measured, and analyzed by paired t-test.
Results
Mediolateral deviation, length of COP movement, and area of COP occupied were increased after fatiguing exercise of the gastrocnemius muscle. Anteroposterior deviation and length of COP movement were also increased, but had low statistical significance.
Conclusion
These findings suggest that the gastrocnemius muscle fatigue affects mediolateral stability and accuracy during single leg standing in elderly people. Therefore muscle endurance training is necessary to prevent falls in elderly people.
INTRODUCTION
Falls in the elderly are a very common and severe problem. As of 2010, the population of elderly aged over 65 years in Korea reached 11% of the total population [1], approximately 35%-40% of whom experience falls more than once a year [2]. More attention needs to be paid to falls in the elderly of higher age due to secondary complications, such as fracture or pain [3]. The experience of falls lowers the confidence of elderly in walking, making it difficult for them to participate in social activities. Elderly falls also increase medical expenditures for complications, resulting in higher personal or social burdens [4].
Postural control is the ability that is necessary to safely perform walking and daily activities and is closely related to falls. Both neurological and musculoskeletal factors are complexly involved in postural control. Neurological factors include central processing and neural pathways for motor control after sensory organs, such as the visual, vestibular and proprioceptive organs, receive some information related to imbalance [5]. In normal conditions, if external factors change, balance is maintained by controlling the dependency on each sense. But in abnormal conditions, such as damage to the peripheral sensory organs or a peripheral neuropathy, the risk of falls increases due to lack of information for maintaining balance. In central neuropathy, balance control ability decreases because it is difficult to properly integrate each sense responding to external changes [6].
Motor signals recover various imbalance conditions whether it is predictable or not [7], or activates the musculoskeletal system to safely perform activities of daily living [8]. The ankle strategy is usually used for slow and small perturbations on a firm and wide surface. If, however, the perturbation becomes larger and faster, both ankle strategy and hip strategy are used to recover balance [5]. The ankle strategy is usually used to maintain balance in daily living activities of, in which the ability for controlling submaximal isometric plantarflexion is more important than that of controlling maximal isometric plantarflexion [8].
Understanding the effects of plantarflexor muscle fatigue on balance control may be helpful for preventing falls that can occur during daily living activities. Yaggie and McGregor [9] reported that when muscles around the ankle become fatigued due to plantarflexion, balance control weakens and the ankle becomes chronically unstable, this causes injuries. Ochsendorf et al. [10] also reported that fatigue of the plantarflexor muscles can weaken balance control and cause ankle injuries. These indicate that muscle endurance around the ankle is closely associated with balance control. These studies, however, were conducted on young adults, and few studies have been available for the effect of muscle fatigue around the ankle on balance control in the elderly who frequently experience falls due to weakened muscle endurance.
This study, therefore, investigates the effects of plantarflexor muscle fatigue on postural control by inducing muscle fatigue with submaximal isometric plantarflexion in normal elderly subjects.
MATERIALS AND METHODS
Materials
The subjects of this study include 24 healthy elderly over 65 years (17 men, 7 women) who perform daily activities independently (Table 1). All subjects having one of the following were excluded: a history of visual or vestibular diseases, peripheral neuropathy or neurological diseases, lesions of the central nerve system that can affect cognitive function, a treatment history for spinal disorder or severe arthritis, musculoskeletal limitation of the range of motion associated with balance control [11], endocrine disorder including diabetes, a medication history affecting balance maintenance, or a history of falls in the recent year.

General characteristics of subjects
Before starting this study, an approval from the Institutional Review Board was granted. Subjects included the elderly who had participated in individual interviews and consented after being given a full description of the objective of the study and testing.
Methods
Assessment of balance control before and after muscle fatigue
The relationship between muscle fatigue and postural control was evaluated by measuring balance control with Health Improvement & Management System (HIMS; The HIMS Inc., Suwon, Korea) posturography before and after fatiguing exercise. For the balance control test, subjects were asked to place one bare foot on the center of a force plate, keeping their eyes straight and putting both hands on their waists in a quiet room with little external stimulation (Fig. 1). Movement of the four limbs that could affect balance control was limited, and four testers were positioned near the subjects to prevent falling. After fully understanding the test method by practicing single leg standing twice before fatiguing exercise, 2 single leg standing tests were performed with 30-second rest between the tests. After the muscle fatiguing exercise, postural control ability was evaluated again with the posturography without any practice.

Postural control ability of single leg standing evaluated with Health Improvement & Management System (HIMS) posturography.
Fatiguing exercise of plantarflexor
QEMG-4 surface electromyogram (Laxtha, Daejeon, Korea) equipped with a 4-channel recording unit was used to evaluate plantarflexor muscle fatigue. The measurement was sampled at the rate of 1,024 Hz, with the frequency set and recorded between 10-2,000 Hz. As for the amplified electromyogram signal, the mean of the root mean square (RMS) was measured after the processes of full wave rectification and 20 Hz high pass filter with the EMG Works program (Laxtha, Daejeon, Korea) [12].
After 5 minutes of warm-up exercises and stretching, subjects sat on a chair with the hip flexed at 80°-90°, knee and ankle positioned at 0°, trunk and thighs fixed, and then practiced isometric plantarflexion exercises (Fig. 2). Before performing the surface electromyogram, the body part of subjects holding the electrode was wiped with alcohol to reduce skin resistance. A small amount of electromyogram gel was applied to the surface electrode (Delsys Ind., Boston, USA), which then was attached to the medial belly of gastrocnemius muscle.
Posture of isometric ankle plantarflexion.
After the warm-up exercise and preparation for surface electromyogram, a test for maximal voluntary contraction (MVC) of the plantarflexor was performed. Without any contraction on the shoulders, trunk, and thighs during the test, three 3-second maximal isometric plantarflexions were performed. A 5-second rest was given between each contraction. The exercise was performed from the left leg to the right. Of the MVC values of both gastrocnemius muscles obtained by the exercises, the maximum RMS value each was defined as 100% muscle activity, 40% of which was set as a criterion for fatiguing exercise (40% MVC) [8,13].
The method of Nordez et al. [13] was used as a reference for fatiguing exercise. Having had a 5-minute resting period, subjects began submaximal isometric plantarflexion at the contraction of more than 40% MVC with the computer monitor watched, and continued it to the point where muscle fatigue was induced. The point of muscle fatigue was defined when 40% MVC value was reduced by more than 5% for 5 seconds during fatiguing exercise, or subjects could not continue the exercise due to fatigue, at which time the exercise was discontinued (Fig. 3).

Subjects undertook fatiguing exercises consisting of warm-up exercise (W), maximal voluntary contraction (MVC) with some contractions (C) and rests (R), submaximal isometric contraction, and end of test (E).
Measurement variables
In order to analyze the difference of balance control before and after muscle fatigue, mean deviation, length and area of the center of pressure (COP) were used (Figs. 4, 5).

Center of pressure (COP) motion was assessed by deviations X and Y, area of COP, and length of COP.
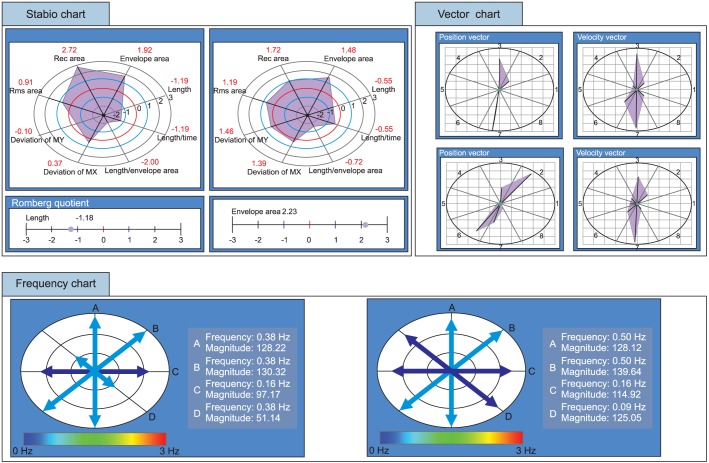
Example of posturography results.
Statistical analysis
SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. All data obtained to examine the change of postural control ability before and after muscle fatigue were described by mean and standard deviation to identify their patterns. The difference of the variables in each group was analyzed by paired t-test. A p-value<0.05 was considered statistically significant.
RESULTS
Mean deviation
The mediolateral and anteroposterior deviations of the subjects' bodies were assessed by analyzing the mean of the COP position toward the x-axis (deviation X) and y-axis (deviation Y) (Fig. 4). Mediolateral deviation (deviation X) increased more after fatiguing exercise (1.98±2.03 cm) than before the exercise (0.97±0.74 cm) (p<0.05). Anteroposterior deviation (deviation Y) increased (1.90±1.95 cm) more after the fatiguing exercise (1.90±1.95 cm) than before the exercise (1.08±1.86 cm), but no statistical significance was found (Table 2).
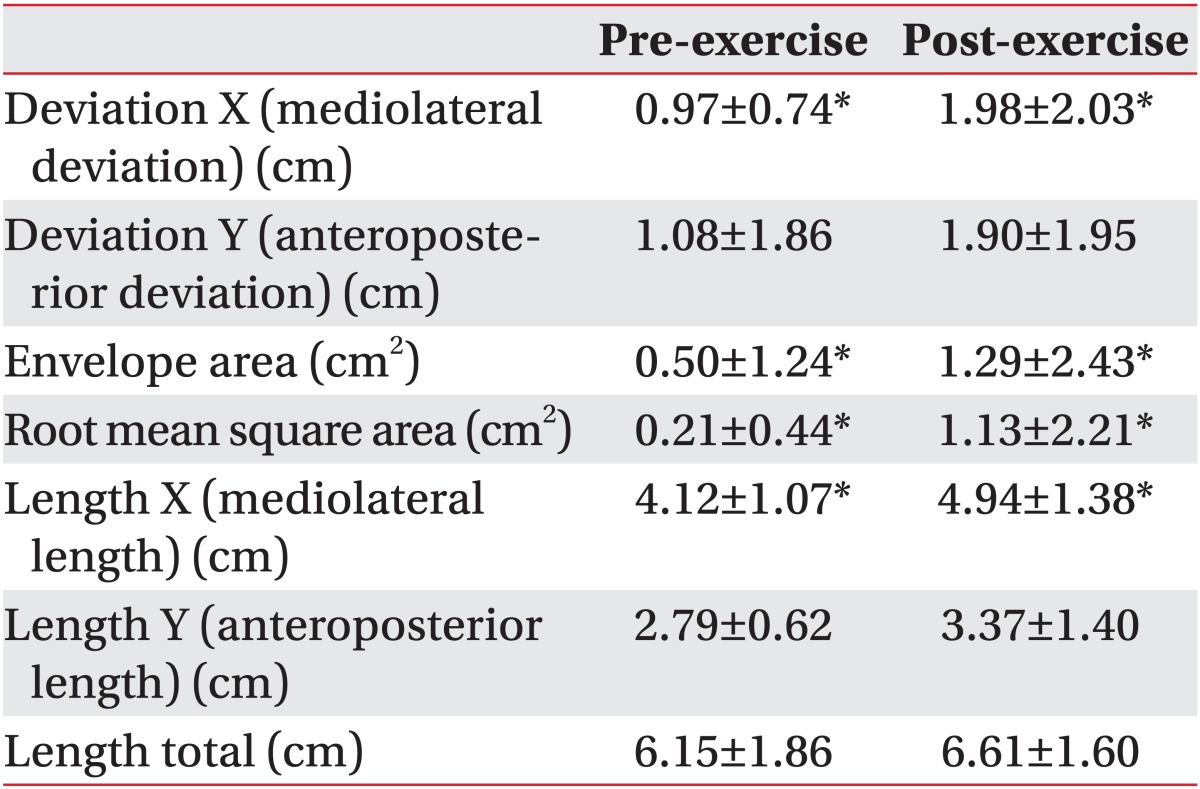
Comparison of deviations X and Y, areas, lengths in pre-exercise and post-exercise
Area
The change in the accuracy of the postural control before and after fatiguing exercise was assessed by analyzing the occupied area of COP with the indices of envelope area (EVAR) and root mean square area (RSAR) (Fig. 4). EVAR increased more after fatiguing exercise (1.29±2.43 cm2) than before the exercise (0.50±1.24 cm2), and RSAR also increased more after fatiguing exercise (1.13±2.21 cm2) than before the exercise (0.21±0.44 cm2) (p<0.05) (Table 2).
Length
Length indicates the length of COP movement toward all directions during the balance test, including the mediolateral and anteroposterior directions, and can be used to evaluate postural sway and the efficiency of postural control ability (Fig. 4). The mediolateral length of COP movement (length X) increased more after fatiguing exercise (4.94±1.37 cm) than before the exercise (4.12±1.07 cm). On the contrary, the anteroposterior length of COP movement (length Y) increased more after fatiguing exercise (3.37±1.40 cm) than before the exercise (2.79±0.62 cm), but had no statistical significance. The length of COP movement in all directions (length total) increased more after fatiguing (6.61±1.60 cm) than before fatiguing (6.15±1.86 cm), but was not statistically significant as well (Table 2).
DISCUSSION
The prevalence of sarcopenia is 30% in the elderly aged over 65 years and 50% in those aged over 80 years [14]. Sarcopenia refers to a series of changes where the type I and type II muscle fibers are lost during the ageing process. The loss of type II muscle fiber is closely related to the weakness of muscle strength, as well as muscle endurance [15]. According to King et al. [8], if muscle endurance weakens, muscles around the ankle get easily fatigued and make it difficult to control submaximal plantarflexion, affecting the activities of daily living. This explains how important muscle endurance of the ankle is for postural control.
Plantarflexion is controlled primarily by the gastrocnemius and soleus muscles, and partly by the plantaris muscle, flexor hallucis longus muscle, flexor digitorum longus muscle, peroneus muscle, and tibialis posterior muscle [16]. Plantarflexion is usually used for ankle strategy: when the center of gravity travels anteriorly during the forward lean, the proprioceptive structures in the plantarflexor, such as the muscle spindle and Golgi tendon organ, are activated and elicit adequate an response, resulting in plantarflexion [9]. Since maintaining balance through the successful control of plantarflexion is important for safely conducting daily activities, this study attempted to induce fatigue on the plantarflexor and investigate what changes occur to postural control.
In the present study, if fatigue was induced to plantarflexor muscles, the mean COP showed more anteroposterior deviation and postural sway became larger, but no statistical significance was found. This finding can be attributed to the fact that compromised balance due to fatigued plantarflexor was compensated by the recruitment of alternate motor unit [9]. According to Gribble et al. [17], muscle damage causes change in the activation of muscle spindle, slows down afferent feedback and contributes to the deterioration of anteroposterior postural control ability in ankle strategy. Exercising protocol at 125% to 150% of maximal isometric force can cause damage to the plantarflexor [18]. In this study, however, since the isometric fatiguing exercise was performed at the submaximal muscle strength of 40% MVC, it could not be sufficient to cause damage to the plantarflexor, and has a limitation to considerably affect balance control.
In this study, the degree of mediolaterally displacement of COP and postural sway increased, showing a statistically significant correlation. This appears to be due to the fact that when performing plantarflexion to induce fatigue, fatigue was also induced to the peroneus muscle, which involves plantarflexion as well, as it was co-contracted with the gastrocnemius [9]. Even though the peroneal muscle partly plays the function of plantarflexion, it primarily acts on the eversion of the ankle [17]. If fatigue is induced to the peroneal muscle due to plantarflexion, muscle latency of the peroneals increases [19], and the reaction time to mediolateral imbalance increases, resulting in a weakened balance control of the mediolateral direction [9]. If postural stability of the ankle weakens due to peroneal muscle fatigue, it can be compensated with the activation of the lumbrical muscle, flexor muscle and extensor muscle of the foot [9]. Since, however, it is not sufficient enough to fully compensate, the mediolateral postural control ability ultimately decreases [9]. Gutierrez et al. [20] reported that plantarflexion affects more on the median frequency and firing rate of the peroneal muscle than the gastrocnemius muscle, resulting in reduced mediolateral postural stability of the ankle. This result is consistent with the present study.
The area occupied by COP has a lower value as postural control is more accurately performed [21]. It can be understood that the reason for the increased area of COP after inducing fatigue to the plantarflexor is that the area including all directions increased, because both the anteroposterior and mediolateral length of COP movement increased.
The weakness of plantarflexor muscle endurance in the elderly due to sarcopenia is a risk factor associated with reduced balance control [5]. Wolfson et al. [22] suggested that when elderly people performed muscle endurance exercises around the ankle by practicing Tai Chi on a long-term basis, their balance control of single leg standing increased and could prevent the risk of falls.
Controlling plantarflexion is important for safely performing activities of daily living for the elderly. If the muscles around the ankle get easily fatigued due to reduced muscle endurance, the control of exercise becomes difficult, readily exposing them to the risk of falls [8]. This study shows that the fatigue of muscles around the ankle in normal elderly subjects is closely associated with decreased balance control. This suggests that including muscle endurance exercises around the ankle in exercise prescription for the prevention of falls in the elderly may be effective to prevent falls.
This study has a few limitations. First, since the number of subjects was not large and the test was performed for elderly aged over 65 years, there is a limitation for the results of this study to be applied to the elderly in various age groups. Second, this study cannot fully reflect the dynamic balance changes, such as standing and walking, because it evaluated the balance in a static condition. Finally, the hip adductors/abductors, in addition to the plantarflexor, can affect the mediolateral balance control. Further studies considering these limitations need to be conducted.
In conclusion, for daily activities of normal elderly, submaximal isometric plantarflexion, which is closely associated with muscle endurance, is important. The findings of this study show that the muscle fatigue induced by plantarflexion reduces the ability and accuracy of mediolateral postural control. This suggests that when prescribing exercises to prevent falls in the elderly, a combination of resistance exercises and exercises to improve the muscle endurance around the ankle is effective.
Notes
No potential conflict of interest relevant to this article was reported.