Effect of the Presence of Brain-Derived Neurotrophic Factor Val66Met Polymorphism on the Recovery in Patients With Acute Subcortical Stroke
Article information
Abstract
Objective
To investigate the effect of brain-derived neurotrophic factor (BDNF) Val66Met polymorphism on the recovery after subcortical stroke, using the modified Rankin Scale (mRS).
Methods
Subcortical stroke patients with copies of BDNF Val66Met polymorphism (n=7) were compared to their controls (n=7) without a copy of BDNF Val66Met polymorphism after matching for initial severity, location and type of stroke. The mRS scores at 1 and 3 months after discharge from the neurorehabilitation unit were compared between the groups.
Results
A repeated measures ANOVA for mRS revealed significant interaction between time and group (F(2, 24) =37.2, p<0.001) and a significant effect of time (F(2, 24)=10.8, p<0.001), thereby reflecting significant differences between the Met allele (+) group and the Met allele (-) group. There was a significant difference in mRS scores at 3 months post-discharge between the two groups (p=0.01) although no difference was evident in mRS scores at 1 month post-discharge between the two groups. There were significant improvements between mRS scores on admission and mRS scores at 1 month post-discharge (p=0.02), and between mRS scores at 1 month post-discharge and mRS scores at 3 months post-discharge (p=0.004) in the Met allele (-) group.
Conclusion
BDNF Val66Met polymorphism may be associated with worse functional outcome in Korean patients with subcortical stroke. Therefore, BDNF Val66Met polymorphism should be considered as an important prognostic factor for recovery and responses to rehabilitation therapies after stroke in Korean patients. There is a need for developing different rehabilitation strategies for the population with BDNF Val66Met polymorphism. Further studies assessing different outcomes for various functional domains of stroke recovery are needed to clarify the role of BDNF Val66Met polymorphism.
INTRODUCTION
Stroke is a major cause of disability worldwide and imposes a great socioeconomic burden [1]. Although it is important to maximize the recovery after stroke for reducing the stroke-related burden, the recovery and response to restorative therapies are highly variable between patients [2]. It has been suggested that identification of the mechanism underlying the variability in recovery after stroke is required to provide more effective and individualized rehabilitation strategies. Recent advances in the understanding of the molecular and genetic mechanisms of recovery after stroke have indicated the possible influence of a specific genetic polymorphism in the variability of spontaneous recovery and responses to post-stroke therapy [2-4].
Brain-derived neurotrophic factor (BDNF) Val66Met polymorphism is one of the most investigated genetic polymorphisms that are known to be associated with the recovery after stroke [2]. BDNF is the most abundant neurotrophic factor in the central nervous system and affects neural plasticity [2]. BDNF Val66Met polymorphism is associated with the reduction in activity-dependent BDNF secretion and brain plasticity [5,6], and might lower the capacity of functional recovery after stroke. The report that 30%-50% of humans have at least one Met allele in the BDNF gene indicates the importance of this polymorphism [7].
Several human observational studies have reported that the BDNF Val66Met polymorphism is associated with worse functional recovery after stroke [8-10]. Cramer and Procaccio reported a possible relationship between the presence of the BDNF Val66Met polymorphism and poorer recovery from onset of acute stroke to 1 month post-stroke [8]. The BDNF Val66Met polymorphism has been associated with worse outcome in patients with unruptured brain arteriovenous malformation and in patients with subarachnoid hemorrhage [9,10].
Although the previous studies included a substantial number of patients, these studies were performed only in western countries with heterogeneous ethnicities and did not consider the lesion location, type (ischemic or hemorrhagic) and volume of stroke as confounders for recovery [8-10]. It is possible that different ethnic groups have different modifiers of gene function and a complex ethnic-specific pattern of gene function would be observed including differential effects of the polymorphism [11]. It has also been suggested that there is an interaction between the genetic polymorphism and environment [12]. Therefore, it is required to investigate the role of BDNF Val66Met polymorphism in the recovery after stroke in a different ethnic group and culture. Furthermore, because lesion location, type and volume of stroke have been associated with the recovery after stroke [13-16], these factors should be considered as confounders to clarify the effect of BDNF Val66Met polymorphism.
In this study, we investigated the effect of BDNF Val66Met polymorphism on the recovery after subcortical stroke using the modified Rankin Scale (mRS). Patients with copies of BDNF Val66Met polymorphism were compared to their controls without a copy of BDNF Val66Met polymorphism after matching for initial severity, location and type of stroke.
MATERIALS AND METHODS
Subjects and study design
Patients admitted to the neurorehabilitation unit from April 2009 to June 2012 after acute (<1 month), first-ever subcortical stroke were recruited. Patients were excluded from the study if they were younger than 18 years of age, displayed increased intracranial pressure or did not provide written informed consent. Thirty-six patients were recruited. All subjects received detailed information about the study and provided their written consent, prior to determination of the presence of BDNF Val66Met polymorphism. mRS as a primary outcome instrument was assessed on admission to the neurorehabilitation unit, at 1 month after discharge and at 3 months after discharge. Following measures were assessed only on admission: the National Institutes of Health Stroke Scale (NIHSS), Fugl-Meyer Assessment (FMA) Scale, Brunnstrom stage, Korean version of Modified Barthel Index (K-MBI), and Korean version of Mini-Mental Status Examination (K-MMSE). MRIcro software (University of Nottingham School of Psychology, Nottingham, UK) was used to measure the stroke volume using diffusion-weighted magnetic resonance imaging (MRI) in ischemic stroke patients and computed tomography (CT) in hemorrhagic stroke patients. Motor evoked potentials (MEP) were measured bilaterally in upper and lower limbs. MEPs were measured in all 4 extremities (in abductor pollicis brevis of upper limbs and in adductor hallucis of lower limbs) using a standard protocol [17]. Reproducible responses with a minimal peak-to-peak amplitude of 200 µV in at least 5 of 10 consecutive trials using a figure-of-eight coil with a MagPro ×100 (Medtronic Inc., Farum, Denmark) were defined as a positive response [18]. All assessments of functional outcomes, stroke volume and MEP were performed blinded to the BDNF genotype. This research protocol was approved by the local Institutional Review Board, and this study was conducted in accordance with the regulatory standards of Good Clinical Practice and the Declaration of Helsinki (World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects, 2000).
Genotyping
Genomic DNA of the clinical samples was extracted using the QIAamp Blood Mini Kit (Qiagen, Valencia, CA, USA). Real-time polymerase chain reaction (PCR) reactions were performed using LightCycler 2.0 (Roche, Indianapolis, IN, USA). Genotyping primers and probes were designed using the LightCycler Probe Design Software 2.0 (Roche). The primer sequences were NF-F 5'-GGTTCAAGAGGCTTGACAT-3' and NF-R 5'-TGTTTGCAGCATCTAGGTAAT-3'. The hybridization probe sequences were NF-A 5'-TTCATTGGGCCGAACTTTCTGGTCCTC-Fluorescein-3' and NF-D 5'-LC Red 640-CCAACAGCTCTTCTATCACGTGTT-Phosphate-3'. PCR was performed in a total volume of 20 µL, with 2.0 µL of a reaction mixture comprising of LightCycler FastStart DNA Master Hybridization (Roche), 0.2 µM of each primer and probe and 2.0 µL of template DNA (50 ng/µL). The amplification protocol for this reaction consisted of 40, 5-second cycles of denaturation at 94℃, 10-second of annealing at 58℃ and 15-second of extension at 72℃. Melting curves were acquired by measuring the fluorescence during a temperature transition from 40℃ to 80℃ at the rate of 0.2℃ per second after 30-second of the first step. Fluorescence data were converted into melting peaks by plotting the negative derivatives of fluorescence with respect to temperature (-dF/dT) as a function of temperature. The presence of the BDNF Val66Met polymorphism was determined according to the sequence-specific melting temperature: 66.5±0.5℃ in the GTG/GTG homozygous sample, 60.5±0.5℃ in the GTG/GTG homozygous sample, and double peaks with two melting points in the GTG/ATG heterozygous sample.
Data analysis
Subject selection for analysis
All 36 participants completed the follow-up assessment at 3 months post-discharge. Eight patients did not have the BDNF Val66Met polymorphism, 21 patients had one copy of the BDNF Val66Met polymorphism and seven patients had two copies of the BDNF Val66Met polymorphism. For the analysis, the patients with one or two copies of the BDNF Val66Met polymorphism were pooled. Therefore, there were two groups for analysis: patients without any copy of the BDNF Val66Met polymorphism (Met allele (-) group) and patients with 1-2 copies of the BDNF Val66Met polymorphism (Met allele (+) group). The patients in the Met allele (-) group were matched with the patients in the Met allele (+) group on a one-to-one ratio according to stroke type (ischemic or hemorrhagic), anatomical lesion involved by stroke (white matter [e.g., corona radiata, internal capsule], basal ganglia, thalamus, pontomedullary, and cerebellum) on diffusion MRI or CT in the acute stage and initial stroke severity represented by NIHSS on admission. For matching of the NIHSS score, a difference in scores of up to four was allowed. Matching was performed by one investigator blinded to results of other outcomes, excluding those of NIHSS, on admission. As a result of matching, seven patients in each group were selected for analysis. The initial MRI images and baseline characteristics are presented in Fig. 1 and Table 1, respectively. One patient with large corona radiata infarction in the no polymorphism group could not be matched due to a high NIHSS score of 18.
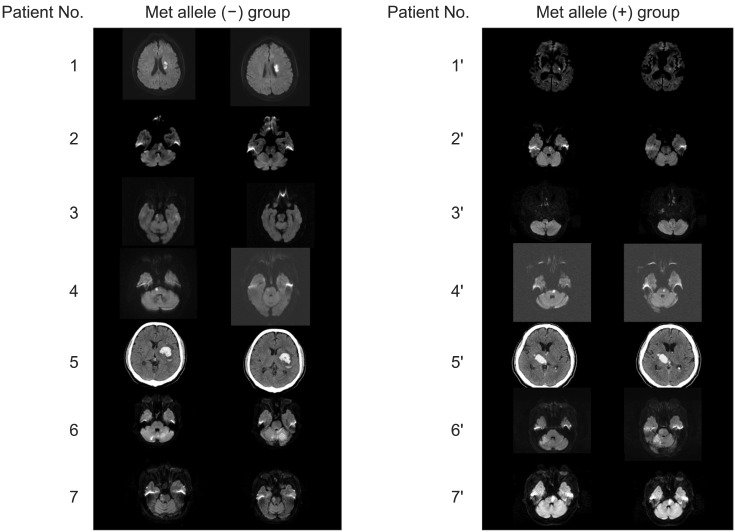
Diffusion weighted magnetic resonance imaging and computed tomography scans (patient 5 and 5') in acute stage of stroke. Patient number with the apostrophe denotes matching of a patient in the Met allele (+) group to the patient with the same number in the Met allele (-) group.
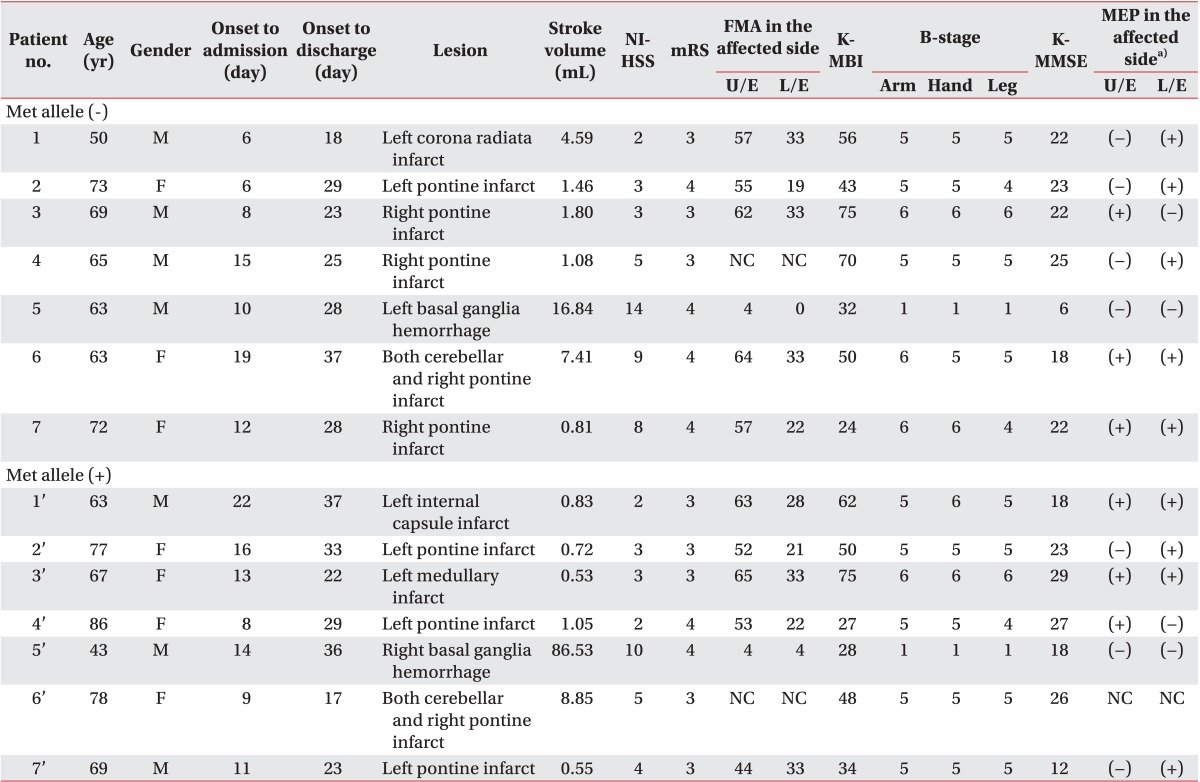
Patients' baseline data according to the presence of brain-derived neurotrophic factor Val66Met polymorphism
Statistical analysis
Continuous variables are presented as the mean±standard deviation for normally distributed data and as the median with interquartile range for skewed data. Categorical variables are presented as frequency (percentage). To compare the baseline characteristics between the two groups, Student t-test or the Mann-Whitney U test (for non-normally distributed data) was used for continuous variables and chi-square test was used for categorical variables. An uncorrected two-tailed p<0.05 was considered statistically significant.
The mRS scores at 1 month after discharge in patients 2 and 3 were not measured and these missing data were imputed by using the last observation carried forward approach. The effect of presence of the BDNF Val66Met polymorphism was evaluated with a repeated measures ANOVA with time (three levels: on admission, at 1 month and 3 months after discharge) as a within-subject factor and group (two levels: Met allele (+) and Met allele (-)) as a between-subject factor. Overall significant differences in time, group and interaction between time and group were determined by a two-tailed p<0.05. Student t-test or paired t-test with Bonferroni correction was applied as a post hoc test only when ANOVA revealed overall significant differences. Student t-tests for mRS were performed at each of the three time points with the significance level of p<0.017 after Bonferroni correction. mRS scores at 1 month and 3 months after discharge were compared to those on admission and at 1 month after discharge, respectively, by the paired t-tests with the significance level of p<0.025 after Bonferroni correction. Statistical analysis was performed using the SPSS PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Characteristics of the patients
Table 1 shows the detailed data of the selected patients for analysis. The two groups were well matched for stroke lesion and type (Table 1, Fig. 1). Patients 5, 6, and 7 had higher NIHSS scores by 4 points compared to those in the matched patients, but the NIHSS score was not different between the other pairs.
There were no significant differences between the two groups in terms of demographic variables, days from stroke onset to admission and discharge and stroke type (Table 2). Among functional outcomes measured on admission, the no BDNF Val66Met polymorphism group showed higher stroke volume, NIHSS, and mRS scores; and lower K-MBI and K-MMSE scores compared to the BDNF Val66Met polymorphism group; however, this difference was not statistically significant (Table 2). No significant differences between two groups were seen in the FMA scale, B-stage, and MEP responses in the affected extremities (Table 2).

Baseline characteristics of patients according to the presence of brain-derived neurotrophic factor Val66Met polymorphism
Differences in recovery according to the presence of BDNF polymorphism measured by the mRS
A repeated measures ANOVA for mRS revealed significant interaction between time and group (F(2, 24)=37.2, p<0.001) and a significant effect of time (F(2, 24)=10.8, p<0.001), reflecting a significant difference between the Met allele (+) group and the Met allele (-) group (Fig. 2). Post-hoc analysis with Student t-test at each time point with Bonferroni correction revealed a significant difference in mRS scores at 3 months post-discharge between the two groups (p=0.01), although no difference in mRS scores was evident at 1 month post-discharge between the two groups (Fig. 2). There were significant improvements between mRS scores on admission and mRS scores at 1 month post-discharge (p=0.02), and between mRS scores at 1 month post-discharge and mRS scores at 3 months post-discharge (p=0.004) in the Met allele (-) group (Fig. 2). In the Met allele (+) group, there were no significant improvements in mRS scores although a trend for improvement was evident (Fig. 2).

Modified Rankin Scale (mRS) on admission to the rehabilitation unit, at 1 month post-discharge and 3 months post-discharge according to the presence of the Met allele. *p<0.017 with Bonferroni correction by student's t-test, †p<0.025 with Bonferroni correction by paired t-test.
DISCUSSION
In this study, we demonstrated that the presence of BDNF Val66Met polymorphism may be associated with worse functional recovery after subcortical stroke in Korean patients. This finding is consistent with the results of previous studies performed in western countries with heterogeneous ethnicities [8-10], thereby suggesting that the BDNF Val66Met polymorphism is a poor prognostic factor for recovery after stroke that can be extrapolated to other ethnic or culture groups despite the possible differential effects of the genetic polymorphism [11,12].
We only included patients with stroke involving the subcortical brain structure in this study. Although some researchers have suggested the possibility that the recovery mechanism of subcortical stroke may be different from that of cortical stroke [19-21], evidence suggests that changes in cortical plasticity are also important for the recovery even after subcortical stroke [22]. Plastic changes around the cortical lesion, which has a functional connectivity with the damaged subcortical area, are associated with recovery after subcortical stroke [23]. Therefore, it seems that BDNF has an effect on the plastic changes in the cortex that are associated with the damaged subcortical area, and a lack of secretion of BDNF in a patient with BDNF Val66Met polymorphism is associated with worse recovery.
Significant differences between the two groups in the recovery measured by mRS were observed at 3 months after discharge from the neurorehabilitation unit, which corresponds to approximately 4 months after stroke onset; and it has been suggested that maximal motor recovery is achieved by plastic changes in the brain during this period [24]. BDNF increases the plastic changes in the brain, which are associated with the recovery of motor, cognitive and speech functions after stroke. Therefore, the differences in BDNF levels that are caused due to the presence of BDNF Val66Met polymorphism can cause differences in the recovery induced by plastic changes in the brain during this period. The reason why there was no significant difference in the function at 1 month post-discharge between groups is unclear. It is possible that the mRS represents a very broad range of function, such that differences in the functional status measured by mRS at that time point could not be detected due to its low sensitivity [25] given the small sample size of our study. Another possible reason is that the initial stroke severity measured by NIHSS was higher in the Met allele (-) group. Patients 4, 5, 6, and 7 in the Met allele (-) group showed a higher stroke severity compared to their controls in the Met allele (+) group (Table 1). Because the initial severity of stroke is related with poor functional recovery, the Met allele (-) group with higher severity of stroke was expected to have a worse mRS score; however, this group showed better functional outcome at 3 months post-discharge. Therefore, it is possible that because of the higher initial stroke severity, approximately 2 months or more were needed for the patients without the Met allele to keep up with the gap of initial stroke severity between the two groups.
This study had several limitations that need to be considered. First, although the two groups were perfectly matched for location and type of stroke, stroke severity measured by NIHSS was not the same between patients 4, 5, 6 and 7 of the Met allele (-) group and their matched cases in the Met allele (+) group, and these patients showed a higher stroke severity compared to their controls in the Met allele (+) group. Because the initial severity of stroke is related with poor functional recovery [26,27], the higher severity of stroke in the Met allele (-) group could be associated with worse mRS; however, a better functional outcome was achieved in the Met allele (-) group. Secondly, three patients (patients 1', 4', and 6') in the Met allele (+) group were substantially older than their matched cases in the Met allele (-) group. Because older age has been considered as a poor prognostic factor for functional recovery after stroke [28], age differences between the groups can lead to the differences in functional recovery. However, there were no statistically significant differences in age between the Met allele (-) group and the Met allele (+) group (Table 2). Furthermore, the above three patients had better values for some prognostic variables of recovery compared to their matched cases. Patient 1' had a lower stroke volume and a better K-MBI score, and patients 4' and 6' had a less severe stroke according to the NIHSS compared to their matched cases. Therefore, we think that the differences in functional recovery according to the presence of Met allele in this study cannot be explained by the substantially older age of three patients in the Met allele (+) group than their matched controls. Thirdly, the sample size was small compared to that in previous studies [8-10]. However, there was a statistically significant improvement in the mRS score only in the Met allele (-) group, and the mRS score at 3 months post-discharge in the Met allele (-) group was also significantly better than the mRS score at 3 months post-discharge in the Met allele (+) group (Fig. 2). This means that the improvement in function was consistent only in the Met allele (-) group, which showed statistically significant changes in the mRS scores despite the small sample size. Fourthly, we only included the mRS as a functional outcome. Although BDNF may also affect the recovery of various impairments after stroke [2,29,30], it was difficult to investigate the possible differential effect of BDNF Val66Met polymorphism with mRS in this study because mRS is a global functional outcome measure [25,31,32]. Fifthly, the one and two copies of BDNF Val66Met polymorphisms were combined into one group for analysis. Although it has been suggested that there is a possible dose-response relationship according to the number of Met alleles, we could not investigate this phenomenon in this study due to the small sample size. Finally, the rehabilitation therapy and patient's medications after discharge were not controlled, which could influence the recovery after stroke.
However, this study has several strengths since many possible confounders for recovery after stroke such as location, type, stroke severity, stroke volume, and motor function measured by FMA and B-stage, cognitive function measured by K-MMSE and corticospinal tract integrity assessed by MEP were initially balanced between the two groups using a matched control and variable functional measurement.
In conclusion, BDNF Val66met polymorphism may be associated with worse functional outcome in Korean patients with subcortical stroke. Therefore, BDNF Val66Met polymorphism should be considered as an important prognostic factor for recovery and responses to rehabilitation therapies after stroke in Korean patients. Furthermore, there is a need for developing different rehabilitation strategies for the population with the BDNF Val66Met polymorphism. Finally, further studies assessing different outcomes for various functional domains of stroke recovery are needed to clarify the role of BDNF Val66Met polymorphism.
ACKNOWLEDGMENTS
This research was supported by SK Chemicals Co. through Seoul National University R&DB Foundation (Grant No. 800-2010095).
Notes
No potential conflict of interest relevant to this article was reported.