Development and Application of a Newly Designed Massage Instrument for Deep Cross-Friction Massage in Chronic Non-Specific Low Back Pain
Article information
Abstract
Objective
To introduce a newly designed massage instrument, the Hand Grip T-bar (HT-bar) and use it to relieve chronic non-specific low back pain (nLBP) through deep cross-friction massage (roptrotherapy).
Method
22 subjects (9 males and 13 females, aged 51.6±6.7) with chronic nLBP were allocated randomly to a Roptrotherapy group (n=12) and a Transcutaneous Electrical Nerve Stimulation (TENS) group (n=10). The Roptrotherapy group received deep cross-friction massage with the HT-bar, which was made of metal and had a cylinder for increasing weight and grooves for an easy grip. It was applied across the middle and lower back for 20 minutes a day, 3 days a week for 2 weeks. The TENS group received TENS for 20 minutes a day, 5 days a week for 2 weeks. The outcome was measured on the pain numeric rating scale (PNRS), by the Oswestry disability index (ODI), and by the Roland & Morris Disability Questionnaire (RMDQ) at pre-treatment, at immediate post-treatment and 2 weeks later. The application of the HT-bar was assessed by a questionnaire to 19 therapists.
Results
At post-treatment, immediately and 2 weeks later, both groups showed significant improvement in PNRS, ODI and RMDQ. During the two weeks after post-treatment, however, the Roptrotherapy group improved in PNRS, ODI and RMDQ, but the TENS group did not. Over 80% of the therapists responded that the HT-bar was useful and comfortable.
Conclusion
This study suggests that deep cross-friction massage can be a beneficial therapeutic technique and that the HT-bar can be a useful instrument in deep cross-friction massage for chronic nLBP patients.
INTRODUCTION
Back pain, which is experienced by 60-90% of the population, is one of the symptoms that is most frequently complained of by outpatients with musculoskeletal diseases in Korea. LBP is defined as pain and discomfort located below the costal margin and above the inferior gluteus folds, with or without referred leg pain. Chronic pain is defined as pain that persists beyond the normal time of healing. Andersson1 defines it as the persistence of pain for 3 months or longer. Various methods have been used for the treatment of low back pain such as physical therapy with modalities like transcutaneous electrical nerve stimulation (TENS), thermotherapy, injection therapy, manipulation, and massage treatment in addition to various medications. Many studies have been done on the effects of these methods.
Massage, one of the oldest forms of treatment, has been described as assisting with circulation and lymphatic drainage, enhancing the elastic and inelastic properties of connective tissue and muscle, fostering relaxation and alleviating muscle pain.2 Today more than 75 types of massage are practiced.2 One massage method is deep cross-friction massage in which the forces are applied perpendicular to the fibers for separating each fiber, mechanically assisting in the alignment of newly formed collagen during healing.2 It has been used to promote local hyperemia, analgesia, and the reduction of adherent scar tissue to ligaments, tendons, and muscles.2 Farasyn et al.3 used the name "roptrotherapy" for the first time. It is a method of deep cross-friction massage with the aid of a bronze T-bar. The investigators concluded that the use of deep cross-friction massage with the aid of a bronze T-bar, starting with 5-10 kg/cm2 is able to deliver force to the deep muscular area so that it regenerates connective scar tissues and reduces muscle hardening after an incomplete inflammatory response and before healing processes reach the repair.3
In massage treatments, therapists often use their hands. According to Hong,4 56.7% of physical therapists complained of pain in one or more body parts, often in the shoulders (29.2%), wrists and fingers (18.7%) and the pain was proportional to the number of patients per day to whom manual modalities were given. Hence, the use of a proper apparatus when performing a massage, which is one type of manual modality, may minimize damage to the therapists. However, an apparatus for the massage treatment of musculoskeletal pain including low back pain has not been developed and studied sufficiently.
On the basis of our experience performing deep friction massages using various conventional massage apparatuses for the treatment of back pain in outpatients and hospitalized patients, we developed a novel type of T-shaped bar ("HT-bar"; Hand Grip T-bar) with which a massage can be effectively performed providing force to the deep muscles and minimizing damage to the therapists. In this study, we applied deep cross-friction massage using the HT-bar to chronic nonspecific low back pain patients and investigated the effects. We then reviewed the evaluations by the therapists who used the HT-bar.
MATERIALS AND METHODS
Subject
People with low back pain for over 3 months and a pain numeric rating scale (PNRS, 0-100) over 30, between the ages of 20 and 65 were included.5,6 Subjects were to mark the PNRS by themselves on a 10 cm ruler that ranged from 0 to 100 where 0 implies 'no pain at all,' and 100 means 'the worst pain imaginable'.5 The exclusion criteria included: acute or subacute low back pain within 3 months, recent low back pain treated within the previous 1 month, history of diabetes or thyroid disease, general disease such as rheumatic disease, pregnancy or breast-feeding, pacemaker or implanted electrical device, suspicious malignancy or thrombosis, scoliosis, vertebral fracture, myopathy, traumatic low back pain, current disc herniation, history of lumbar surgery, neurological problems of the central or peripheral nervous systems.6,7
Twenty-six patients were recruited. One with a history of lumbar surgery and another with a history of a recent injury were excluded after an interview. The remaining 24 patients were randomly divided into the Roptrotherapy group and the TENS group.
A newly designed T-bar
T-bars that are used as an apparatus for massages are made of various materials, and most of them have two bars connected to each other in a T-shape. We fabricated a T-bar with metal and increased the weight (weight=0.325 kg) by adding a metal cylinder at the central part so that therapists may apply greater pressure with less power from the shoulders and wrists compared to conventional apparatuses. To make the grip of the apparatus more convenient, we modified the conventional handle, which was a simple linear bar, by making the diameter at the middle of the handle (4.5 cm) greater than that at both ends and attaching a metal cylinder beneath the handle (1.3 cm). Grooves were made at the bottom of the cylinder so that they could be wrapped with the index finger and the middle finger or with the middle finger and the ring finger. The entire handle was covered with PVC (Polyvinyl chloride), and one layer of the sponge was overlapped on the region that is in contact with the palm to reduce the fatigue of the hand by decreasing the resistance (counterforce) on the palm when providing pressure with the T-bar. The handle was also covered with leather to provide a soft feeling and increase user convenience. The longer the vertical pillar is, the higher the risk of damage from wrist hyperextension or hyperflexion when applying perpendicular force to the skin surface. Therefore, the length of the vertical pillar including the length of the metal cylinder was minimized to increase the stability. The tip of the bar that contacts the patient's skin was covered with rubber to minimize the stimulation at the time of skin contact (Fig. 1).

Hand grip T-bar (HT-bar) was made of metal and had a metal cylinder (diameter=2.7 cm, height=3 cm) and grooves in middle of vertical bar, just below the cylinder. Both side of the horizontal bar was wrapped by polyethylene rubber pipe and blue sponge in 3 mm was placed above it; then the whole area of the horizontal bar and top of the cylinder which is in contact with the palm were overlapped in leather. Anterior (A), Superior (B), Lateral (C) view of HT-bar.
Intervention
The patients were randomly divided into two groups. In the Roptrotherapy group, deep cross-friction massage was performed for 20 minutes with the HT-bar at both the thoracolumbar regions (T6-L3) and hip muscles including the region where the patients complained of pain.3 The therapy was performed by two therapists and the pressure was maintained at a level that the patients were able to endure within the range of 5-10 kg/cm2. Before performing the massage, the therapists learned how to apply sufficient pressure by watching the pressure level with a pinch gauge.10 The therapy was performed a total of six times over two weeks, three times a week with two-day rest intervals.3,11 In the TENS group, high frequency electrical stimulation was continuously applied high frequency stimulation (100 Hz, rectangular 250 µs pulses)8 using a two channel portable TENS eco 2® (Schwa medico, Ehringshausen, Germany). Two surface electrodes were attached to the regions where the patients felt pain,9 and the maximal intensity electrical stimulation tolerable to the patients was applied.11,12 The stimulation was performed a total of ten times over two weeks, five times a week, for twenty minutes at a time. No other treatment was implemented in either group.
Outcome measures
The Pain Numeric Rating Scale (PNRS), Oswestry Disability Index (ODI), and the Roland Morris Disability Questionnaire (RMDQ) were used as instruments to assess low back pain and to evaluate the effects on the pain and functions. The ODI is composed of ten questions, five points for each question, and the total score is expressed as a percentage.7 The RMDQ is composed of 24 questions and a higher score on the 24-point scale indicates a more severe level of disability.13 The RMDQ was reported to closely reflect the variation over time in patients with back pain.14 The assessment was performed three times: before the treatment, immediately after the treatment, and two weeks after the treatment completion. To compare the therapeutic effects between groups, we (i) analyzed differences between before and immediately after treatment, (ii) differences between before treatment and two weeks after treatment, and (iii) differences between immediately after treatment and two weeks after treatment (Fig. 2).

Flow chart of the study.
Response of the therapists about the HT-bar
A questionnaire was given to the therapists with respect to the usefulness, effect, and convenience of the HT-bar in order to compare it with conventional massage apparatuses. The therapists had experience using the conventional T-bar, and they provided answers to the questionnaire after using the HT-bar more than five times (Appendix).
Data analysis
All statistical analysis used the SPSS14 program. The Mann-Whitney test was used to compare group age, duration and initial data for PNRS, ODI, and RMDQ. A χ2-test was used to compare group gender. A Wilcoxon signed rank test was used to compare the effect between baseline and immediate after treatment, and baseline and 2 weeks after cessation of treatment in each group. A p-value less than 0.05 were considered statistically significant.
RESULTS
General characteristics of subjects
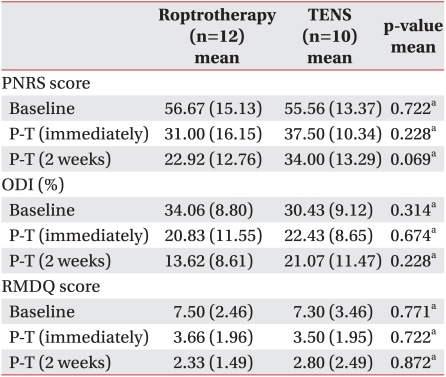
All 24 subjects were enrolled in the study, but two were not able to finish, one because of an ankle sprain and another for personal reasons. The remaining 22 subjects who participated were examined. Twelve patients (7 females and 5 males) were in the Roptrotherapy group. Their mean age was 50.25±6.69 years, mean duration of pain was 9.08±5.06 months. Ten patients (6 females and 4 males) were in the TENS group. Their mean age was 53.30±6.67 years, and mean duration of pain was 8.80±5.55 months. There was no significant difference between the two groups in age, duration of pain, gender, PNRS, ODI, and RMDQ at baseline (Table 1, 2).
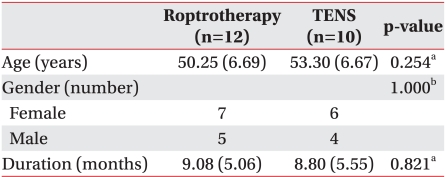
Baseline Characteristics
Comparison of the Variables between Baseline and Post-treatment
Comparison of the results in each group before and after the treatment
Both the Roptrotherapy and the TENS groups showed a significant decrease in PNRS, ODI, and RMDQ scores immediately after the treatment and two weeks after the treatment when compared with the scores before the treatment (p<0.05). The TENS group did not show a significant difference between PNRS, ODI, and RMDQ scores immediately after the treatment and two weeks after the treatment (p>0.05), whereas the Roptrotherapy group showed a significant decrease in scores for all three instruments (p<0.05) (Table 2) (Fig. 3).
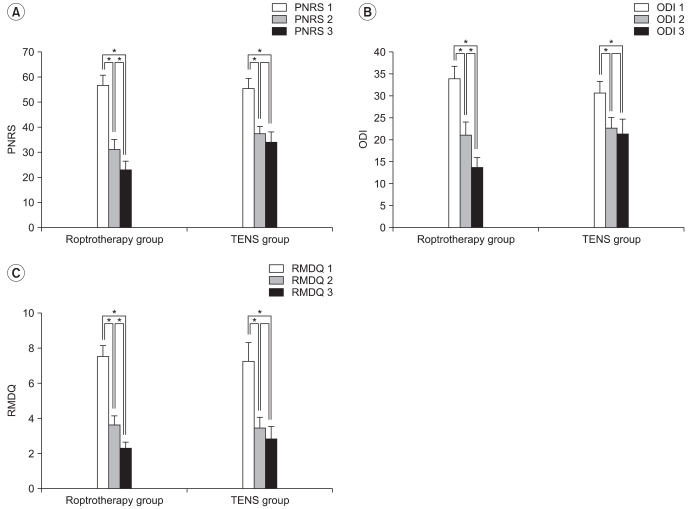
The post-treatment immediately and 2 weeks later, scores of PNRS, RMDQ and ODI were decreased significantly in both groups. Comparing post-treatment immediately and 2 weeks later, there were significant changes of PNRS, ODI, RMDQ scores in the Roptrotherapy group, but no significant change in the TENS group. PNRS: Pain numeric rating scale, ODI: Oswestry disability index, RMDQ:Roland & Morris Disability Questionnaire. *p<0.05.
Comparison of the therapeutic effect between the two groups
There was no significant inter-group difference between the initial measurement values and the measurement values immediately after the treatment. However, compared to the TENS group, the Roptrotherapy group had significantly greater decreases in ODI scores in the following two chronological comparisons: the one between the initial measurement and the measurement two weeks after the treatment; the other between the measurement immediately after the treatment and the measurement two weeks after the treatment (Table 3) (p<0.05).
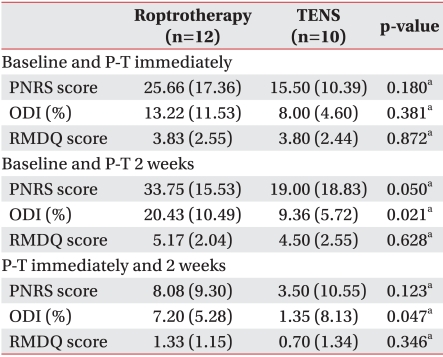
Comparison of the Change between Baseline and Post-treatment
Comparison of the improvement in each group based on the percent change two weeks after the treatment
The percent change, which is the ratio of the measurement values after two weeks to the initial measurement values, was judged as no change if the change was less than 25%, as good if the change was 25% or higher and less than 75%, and as excellent if the change was 75% or higher. It was used to compare improvement depending on the therapeutic methods. With respect to all the scales, the ratio of the patients who showed a change of 'good' or more was higher in the Roptrotherapy group than in the TENS group and the ratio of patients who showed no change was much lower in the Roptrotherapy group than in the TENS group (Fig. 4).
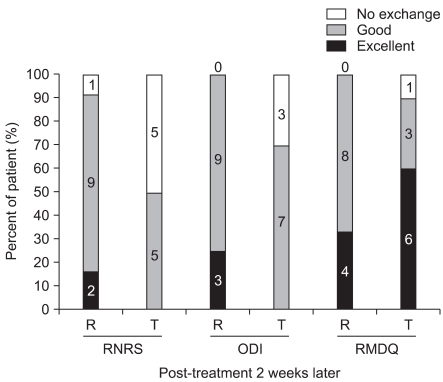
Post-treatment 2 weeks later, the percentage of patients with scores of good or excellent in the Roptrotherapy group was higher than in the TENS group according to all evaluation tools. Values shown in the bar graph are the number of cases. R: Roptrotherapy group, T: TENS group, PNRS: Pain numeric rating scale, ODI: Oswestry disability index, RMDQ: Roland & Morris Disability Questionnaire.
The result of the questionnaire regarding the HT-bar
Nineteen therapists whose average clinical experience was 9.26±6.36 years completed the questionnaire. For question 1, three (16%) therapists chose No. 3, seven (37%) chose No. 4, and nine (47%) chose No. 5. For question No. 2, one (5%) therapist chose No. 3, eight (43%) chose No. 4, and ten (50%) chose No. 5. For question No. 3, one (5%) therapist chose No. 1, two (11%) chose No. 2, and sixteen (84%) chose No. 5.
Abnormal reaction
During this study, none of the patients showed any abnormal reactions that can be expected due to the electric stimulation therapy including skin complications such as skin burn or hypersensitivity, pain by electric stimulation, and excessive muscular fatigue. One patient complained of skin discomfort at the early stage of the first session of the deep cross-friction massage using the HT-bar, but the patient did not complain of any discomfort from the second time on. No other side effect was observed.
DISCUSSION
Massage has been widely applied as therapy for pain, connective tissue injury, muscle soreness and hypertonicity since its therapeutic effect has been recognized. However, compared to the frequency of use and the long history, there are only a limited number of scientific reports on the effects of massage. One generally accepted hypothesis is that a tactile signal is transmitted through large diameter myelinated fibers when performing a massage, resulting in the blockage of pain signals. In addition, it is assumed that the blood circulation in the soft tissues is increased, thus enhancing the excretion of lactate or inflammatory substances and facilitating secretion of endogenous opiates. Furthermore, physical contact decreases pain by means of a psychological effect (a well-being sensation).2,15
Regarding the back pain-reducing effect of massage, Melzack et al. conducted a comparative study with 41 patients who had had low back pain for 36.2 weeks on average, dividing them into two groups. One group received gentle massages using four suction cups to which a little negative pressure was applied. The massages were performed two times a week for 30 minutes each time for a total of ten times. The other group received TENS therapy for the same duration and same number of sessions. They reported, based on the result of the test, that immediately following the therapy, the TENS therapy was more effective than that of the massage therapy in relieving pain and increasing the range of motion and the straight leg raising test result. Furlan et al.16 reported that massage was inferior to manipulation and TENS, equal to corsets and exercises and superior to relaxation therapy, acupuncture and self-care education. It was concluded that massage might be beneficial for patients with subacute and chronic nonspecific LBP in systemic review. They concluded that the massage was less effective than TENS, but only a few of the studies reviewed in the meta-analysis mentioned massage specifically. Most of the massages specifically described were superficial massage methods such as kneading.
Farasyn et al.3 performed deep cross-friction massage using an apparatus with 60 patients with subacute nonspecific low back pain and reported a significant decrease in back pain. This study was conducted by dividing the subjects into the Roptrotherapy group in which the deep muscles were stimulated, the ender mology group in which stimulations were given only to the endodermis with LPG® (LPG systems, Valance, France), and a non-therapy group in which no therapy was provided. In the follow-up test performed one week later, only the Roptrotherapy group showed a significant decrease in pain sensitivity, pain index, and disability.
Deep cross-friction massage in which the forces are applied perpendicular to the fibers in an attempt to separate each fiber,2 mechanically, promotes local hyperemia, analgesia, and reduction of adherent scar tissue to ligament, tendon and muscle structure.17
Macgregor et al.18 applied transverse friction massage to the calf muscle of patients with spastic diplegia and reported that, after massage, the amplitude of voluntary alternating ankle rotation increased and motor skill was improved. They suggested that massage resets sarcomere lengths and redistribution of sarcomere lengths within muscles could have reset proprioceptive feedback. Increased tension of the muscles around the lumbar spine, chronic muscle contraction, and muscle fatigue are commonly found in chronic low back pain patients.19 It can be explained as the result of trunk muscle atrophy and stiffening of the ligaments and joints by the pain and the consequent reflective suppression. This reduces the patient's activity more, enhancing muscular stiffness and sprain and thus exacerbating the pain.20
When performing deep cross-friction massage, the prolife ration of fibroblasts is facilitated, as pressure applied to the muscle is higher, resulting in the facilitation of soft tissue healing and realignment.21 Hence, more force is required for effective therapy, and thus, the physical load on the therapists increases. In this regard, Davidson et al.22 suggested that use of a specially designed apparatus could provide more force to the soft tissues than the force applied by the fingers and thus increase healing of the damaged regions by enhancing the recruitment of fibroblasts. A T-shaped bar is used in order to reduce the pressure on the fingertips of therapists when performing massage therapy by applying force to the deep tissues, to prevent damage by avoiding overuse of the hands, and to elevate the therapeutic effect by applying sufficient pressure at the same time. However, the conventional T-shaped bar still requires great force from the shoulders and wrists to deliver the force to the deep tissues such as the deep muscles of the lumbar spine. Therefore, we invented a T-shape metal bar with a cylinder at the center so that the weight of the bar itself could be heavier than a conventional one and thus provide pressure to the deep muscle region, reducing the force required by the therapists. The area of the rubber part that is in contact with the skin is similar to the tips of the thumbs that are in contact with the skin when the therapists do a massage. The boundary line of the rubber tip was softly curved so that the pressure delivered to the skin when applying force may be progressively distributed from the center to the outer region. Since the handles of most conventional T-shaped bars are simple bar types, fatigue accumulates in the wrists and fingers (Fig. 2). Hence, we modified the handle to make the grip more comfortable and covered it with a material that can disperse the pressure at the skin-contacting region.
More than 80% of the respondents to the questionnaire on the newly developed HT-bar in this study answered that it is a useful apparatus, effective in treating patients, and more convenient than conventional massage apparatuses, indicating that results met the developmental purpose of the HT-bar.
In the Roptrotherapy group where deep cross-friction massage was performed with pressure as high as 5-10 kg/cm2 using the newly developed HT-bar for chronic back pain, a significant decrease in pain and disability was found not only immediately after treatment, but also, two weeks after treatment. This was consistent with the results of conventional studies on the physiological effect of deep cross-friction massage. The transverse friction massage which was applied to the deep muscular layer with high pressure might have stimulated small muscles in the deep lumbar region such as lumbar multifidus and rearranged the pattern of muscle fibers that was causing the chronic muscle tension. This means that muscular tenderness at this level reverted to a less pathological condition after a Roptrotherapy session.3
Since there is little previous research on Roptrotherapy, we referred to the following studies in order to select the appropriate comparative tools for the control groups in this study. According to the Cochrane review by Khadilkar et al.,23 the effects of TENS have been verified for a long period of time, providing good evidence of reducing back pain, although it is limited in discussing the effect of TENS as a therapeutic tool for back pain. There are also studies where ice massage and TENS were applied to patients with knee osteoarthritis or back pain,24,25 a study where soft tissue massage and TENS were applied to patients with neck pain,26 and the abovementioned study where massage using suction cups and TENS were applied to patients with low back pain.11 Considering these studies, we selected TENS as the comparison treatment method.
Several parameters can be chosen when performing TENS therapy. Kim et al.27 and Ghoname et al.28 reported that low frequency acupuncture-like electric nerve stimulation was effective in alleviating pain. Melzack et al.11 and Yurtkuran and Kocagil24 applied low frequency TENS to patients with chronic low back pain and to patients with knee osteoarthritis, and reported a significant pain decrease. Yokoyama et al.29 applied alternating 4/30 Hz frequency TENS to chronic low back pain patients and found a significant decrease in pain from eight weeks of therapy. Deyo et al.30 and Marchand et al.31 applied high frequency TENS to patients with chronic low back pain and reported a significant decrease in pain. In particular, Marchand et al.31 applied high frequency (100 Hz, 125 µs) TENS with low intensity signals for ten weeks, two times per week, reporting that there was a significant decrease in pain immediately after the therapy and one week after the therapy, but the effect was not maintained by the sessions three months and six months after the therapy. Warke et al.32 applied low frequency (4 Hz, 200 µs) TENS and high frequency (110 Hz, 200 µs) TENS to multiple sclerosis patients with chronic low back pain for a total of six weeks, two times per week for 45 minutes at each session. They reported that the pain alleviating effect was the greatest in the group in which high frequency TENS was applied, but the follow-up test performed 32 weeks after the therapy showed that a long-term effect was found only in the group in which low frequency TENS was applied. Graff-Radford et al.8 applied TENS to groups with four different modes and used a placebo group to evaluate the effect of TENS on myofascial pain and trigger point sensitivity. They reported that the most significant decrease in VAS and PTT was found in the high frequency (100 Hz, 250 µs) TENS group. Regarding the intensity of the TENS therapy, Aarskog et al.33 applied high frequency (100 Hz) TENS and Claydon et al.34 applied high frequency (110 Hz) and low frequency (4 Hz) TENS at two different intensity levels. They reported that the pain-reducing effect was greater at the higher intensity level and concluded that high-intensity current is the most important parameter of TENS in connection with the therapeutic effect. In our study, the follow-up period after the treatment was two weeks. High frequency electric stimulation therapy was shown to be effective in chronic low back pain patients in previous studies where the same follow-up period was used. Thus, we selected the following parameter for the TENS group: 100 Hz, 250 µs and at the maximal intensity tolerable to the patients. In the TENS therapy group, the pain was significantly reduced after the therapy compared with before the therapy, which was consistent with the results of previous studies. On the other hand, comparison of the results of the Roptrotherapy group and the TENS group showed that the overall result was better in the Roptrotherapy group. This difference may be because the deep cross-friction massage therapy in this study was applied with sufficient pressure by means of the newly developed HT-bar apparatus that provided not only the general effects of the massage therapy in pain alleviation but also changes in the physiological states of the soft tissues and connective tissues. This is different from the superficial or gentle massage performed in the previous studies11,16 where the effects of massage and TENS were compared with each other.
The limitations of our study are that there was no non-treated group, that the effect of manual massage by the therapists and the massage using the conventional T-shaped bar were not compared, that generalization is difficult because the number of subjects was small, and that no evidence that can verify clinical experiences could be provided, as in other studies, because low back pain was measured as a subjective state.13
It will be necessary in the future to conduct a study that compares Roptrotherapy to a non-treated group in addition to a study that analyzes the effects of reducing patients' pain and disability. The pros and cons that therapists feel by comparing conventional manual massage therapy, massage therapies using other apparatuses, and TENS therapy in various modes should also be studied. It will also be necessary to conduct a study that examines the long-term effects of Roptrotherapy during a sufficiently long follow-up period.
CONCLUSION
Deep cross-friction massage using the HT-bar was equal to or more effective in relieving the pain of chronic nonspecific low back pain patients and reducing their disability than with TENS therapy, and the continuity of the effect was better after the end of the treatment. The usefulness and convenience that the therapists experienced when using the HT-bar were greater than when using a conventional apparatus. Therefore, application of deep cross-friction massage with the HT-bar for the treatment of patients with chronic, nonspecific low back pain will help to decrease pain experienced by patients, reduce their disability, and decrease fatigue of the therapists.
ACKNOWLEDGEMENTS
This study was supported by a grant of the Korea Healthcare Technology R&D Project (A091220), Ministry for Health, Welfare & Family Affairs, Republic of Korea.
Appendices
Appendix
Questionnaire for Hand Grip T-bar (HT-bar).
