Reliability and Usefulness of the Pressure Pain Threshold Measurement in Patients with Myofascial Pain
Article information
Abstract
Objective
To assess the usefulness of a pressure algometer to measure pressure pain threshold (PPT) for diagnosis of myofascial pain syndrome (MPS) in the upper extremity and trunk muscles.
Method
A group of 221 desk workers complaining of upper body pain participated in this study. Five physiatrists made the diagnosis of MPS using physical examination and PPT measurements. PPT measurements were determined for several muscles in the back and upper extremities. Mean PPT data for gender, side, and dominant hand groups were analyzed. Sensitivity and specificity of Fischer's standard method were evaluated. PPT cut-off values for each muscle group were determined using an ROC curve.
Results
Cronbach's alpha for each muscle was very high. The PPT in men was higher than in females, and the PPT in the left side was higher than in the right side for all muscles tested (p<0.05). There was no significant difference in PPT for all muscles between dominant and non-dominant hand groups. Diagnosis of MPS based on Fischer's standard showed relatively high specificity and poor sensitivity.
Conclusion
The digital pressure algometer showed high reliability. PPT might be a useful parameter for assessing a treatment's effect, but not for use in diagnosis or even as a screening method.
INTRODUCTION
In modern industrial society, simple and repetitive operations have gradually increased due to the influences of production and office automation. An example of such operations is visual display terminal (VDT) work, that can be mentally stressful and requires the maintenance of a fixed body posture with respect to the upper limbs. Several studies have reported that VDT work may cause musculoskeletal disorders including fatigue, pain, asthenia, edemas, and dysesthesia of the neck, shoulders, arms, hands, and other locations.1,2 Such musculoskeletal symptoms are also called VDT-induced cumulative trauma disorders. Musculoskeletal symptoms have a variety of causes and vary widely among individuals. Musculoskeletal symptoms have features (e.g., chronic courses) similar to those of chronic degenerative diseases.3 Myofascial pain syndrome, a musculoskeletal disease, causes continuous pain in the musculoskeletal system and is common among normal office workers who spend large amounts of time performing VDT related tasks. Myofascial pain syndrome is characterized by pain at particular sites, pain at corresponding muscles, referred pain, reduced joint motion, and other symptoms.4
For diagnosis of myofascial pain syndrome, it is important to measure muscle tenderness. Tenderness has conventionally been measured by triggering or pressurizing muscles.5 Pressure algometers are designed to measure deep pressure pain thresholds or tenderness resistance. When a particular site of the body is pressed with a rubber disk having an area of 1 cm2, the device displays the pressure.
Pressure algometers are advantageous for quantifying the pressure pain thresholds of muscles. This quantification concept was raised by Libmann in 1934, and normal pressure pain thresholds in skeletal muscles of the body have been measured since the 1980s. Thereafter, pressure algometers have been widely used in clinical practice. The dolorimeter, that employed scales to measure applied pressures was the first algometer device developed. Since then, pressure algometry using this instrument has been widely employed to evaluate myofascial pain syndrome and various musculoskeletal diseases.6 Standards were established for the pressure pain thresholds of patients with myofascial pain syndrome. For example, the pressure pain threshold of a patient was judged to be abnormal when the pressure pain threshold of a certain site was at least 2 kg/cm2 lower than that of the opposite site, or was lower than the normal value, or was not >3 kg/cm2. In recent years, digital pressure algometers have become the standard, and computer-controlled pressure algometers are currently being developed.
Pressure pain thresholds measured by pressure algometry may produce different results depending on such factors as sex, investigator, and apparatus. Numerous studies have reported lower pressure pain thresholds in females than in males.7-10 The reliability of pressure pain thresholds according to raters or measurement frequencies is relatively high. According to studies published by Chung et al.11 and Chesterton et al.,12 high intra-class coefficients ranging from 0.9 to 0.95 have been reported, implying very high reliability. Errors resulting from measurement devices used were not significant. Dagtekin et al.13 reported in 2007 that a newly developed pressure algometer exhibited consistent measured values compared to established devices and did not show any significant difference from pressure pain thresholds measured with a force plate. In 2009, Kinser et al.14 reported that no difference was found in measured value between a new manometer to which a computer was attached to apply a constant pressure and a general digital manometer.
The objective of this study was to assess the usefulness of a pressure algometer to measure pressure pain thresholds in the upper limbs and the upper part of the body in subjects suffering from myofascial pain syndrome; a musculoskeletal disease common among normal office workers performing large amounts of VDT related work.
MATERIALS AND METHODS
Materials and methods
Five clinicians, each with at least ten years of experience in the department of rehabilitation participated in this investigation involving 222 office workers for National Health Insurance Corporation Company.
The subjects responded to questionnaires concerning their general characteristics. Detailed medical examinations administered by interviews and physical examinations were conducted for the subjects. Based on the diagnosis standard presented by Simons et al.15 in 1999, the subjects were diagnosed as having myofascial pain syndrome when they felt pain at local sites, had short taut bands formed in skeletal muscles around the sites, felt pain when the skeletal muscles were pressed, had pain trigger points causing referred pain at relatively accurate spots around the skeletal muscles, and suffered from limited joint motion because of such pain.
Pressure pain thresholds in 8 muscles, including the bilateral trapezius, infraspinatus, extensor carpi radialis, and extensor indicis proprius muscles of each subject were measured using a digital pressure algometer, FDX® (Wagner instrument, Greenwich, USA). The results were compared and analyzed.
The pressure pain threshold measurements for the trapezius, infraspinatus, and extensor carpi radialis muscles were performed at the center of the upper trapezius, at a position 2-3 fingers below the center of the spine of scapula, and at a position 3-4 fingers below the lateral epicondyle of the humerus, respectively. The pressure pain threshold of the extensor indicis proprius was measured by pressing toward the medial side of the radius from a position 3 fingers above the radial styloid process. The investigator placed the digital pressure algometer on a site to be inspected and pressed against the tester in a vertical direction while increasing the force at a constant rate of 1 kg/cm2. The investigator instructed the subjects to express pain either by saying "ouch" or raising their hands when only slight pain was felt. After all 8 muscles were investigated, the subjects were allowed to rest for 5 min. This procedure was repeated a total of 3 times.
The same investigator analyzed the reliability of the pressure algometer by measuring the pressure pain thresholds in the respective muscles of the subjects 3 times and calculating the measured values as a Cronbach's alpha.
Analysis was performed based on comparisons between the pressure pain thresholds in the right and left sides, sexes, and dominant and non-dominant sides, to determine whether there were statistically significant differences between the pressure pain thresholds.
In the sensitivity and specificity analysis of diagnosis by the pressure algometer, a case where the threshold was ≤3 kg, or the difference in threshold between both sides was ≥2 kg, was considered myofascial pain syndrome as based on Fischer's method. This was compared with the diagnosis of myofascial pain syndrome made by physical examination and diagnostic standards to analyze whether the pressure algometer is a useful tool for the diagnosis of myofascial pain syndrome and the identification of therapeutic effects. In this study, we calculated and proposed a new standard for pressure pain threshold (cut-off value) that provides higher sensitivity and specificity than Fischer's method.
Statistical analysis
In this study, SPSS for Windows version 13.0 used for statistical analysis. The difference in the pressure pain thresholds of the right and left sides, sexes, and dominant and non-dominant sides was analyzed using an independent two-sample t-test. The point where a value obtained by adding the specificity and sensitivity to a peak having coordinates farthest vertically from the baseline when the ROC curve reaches a maximum was set as a cut-off value of the pressure pain thresholds in the corresponding muscle.
RESULTS
General characteristics of subjects
The subjects consisted of 113 males and 108 females (mean age: 43.2 years). The subjects spent an average of 7.3 hr per day working at the computer. Two hundred seven of the 222 subjects used their right upper limbs, which belong to a dominant group, 10 subjects used their left upper limbs, and 5 subjects used both upper limbs. That is, the subjects predominantly used their right upper limbs. The distribution of the subjects according to the location of muscle pain was as follows: 109, 58, and 55 subjects for the right, left, and both sides, respectively, demonstrating that the number of subjects suffering right-side pain was 2-fold greater than the number suffering left-side pain (Table 1).

General Characteristics of Subjects
Prevalence rate of myofascial pain syndrome
One hundred fifty-six of the 222 subjects were diagnosed as suffering from myofascial pain syndrome by the clinical diagnosis standard.
Reliability of pressure algometer
The intra-rater reliabilities (Cronbach's alpha: 0.94-0.98) of the pressure algometer were very high for all muscles tested (Table 2).

Intra-rater Reliability; Cronbach's Alpha of Each Muscle
Analyses of pressure pain thresholds
In the investigation of pressure pain thresholds in each subject, the highest pressure pain threshold (3.6±1.8) was measured in the right extensor carpi radialis, and the lowest pressure pain threshold (4.9±1.9) was measured in the left extensor carpi radialis. In all of the 4 muscles, the pressure pain thresholds in the right sides were statistically significantly lower than those in the left sides (Table 3). However, there was no statistically significant difference between the dominant and non-dominant sides. In all muscles, the pressure pain thresholds measured in the male group were statistically significantly higher than those measured in the female group.

Pressure Pain Threshold of Each Muscle
Sensitivity and specificity to myofascial pain syndrome diagnosed by pressure algometer
Sensitivity and specificity of diagnosis of myofascial pain syndrome were analyzed based on Fischer's method. The extensor indicis proprius was excluded from the analysis because myofascial pain syndrome does not often occur in the extensor indicis proprius. Sensitivity and specificity in the other 6 muscles were analyzed and compared. The specificity in each muscle was determined to be relatively high: 55% for the trapezius, 70% for the infraspinatus, and 80% for the extensor carpi radialis. However, very low sensitivities of -42%, 30%, and 5% were found in the trapezius, infraspinatus, and extensor carpi radialis muscles, respectively. Based on the new pressure pain threshold standard with high sensitivity and validity using the ROC curve, the lowest value (3.35) was measured in the right infraspinatus, and the highest value (4.69) was measured in the right extensor carpi radialis (Table 4).
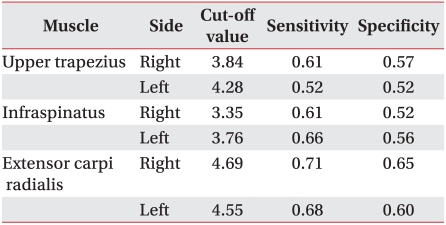
Cut-off Value, Sensitivity, and Specificity of Each Muscle
DISCUSSION
Pressure algometry has been used for the evaluation of pain, the determination of therapeutic effects, and follow-up surveys of treatment in many musculoskeletal diseases.7 However, this technique may be influenced by such factors as inter-observer reproducibility, sex, and dominant and non-dominant sides.
Many reports have been published outside Korea on the pressure pain thresholds of various skeletal muscles. However, research efforts in Korea are still insufficient and their results are also different. Different units such as ounces, pounds, and kilograms were used for pressure pain thresholds in the following papers. For direct comparison of the results, pressure pain thresholds of the trapezius and infraspinatus, as representative muscles, were converted to kg/cm2. Fischer7 reported pressure pain thresholds of 3.7 kg/cm2 and 5.4 kg/cm2 in normal adult females.6 Han et al.3 examined pressure pain thresholds in 95 normal young Korean adults and reported values of 0.8 kg/cm2 and 0.6 kg/cm2, which are very different from values in other reports. Furthermore, Lee et al.8 reported pressure pain thresholds of 2.3 kg/cm2 in 904 female telephone operators, and Lee et al.16 reported pressure pain thresholds of 3.1 kg/cm2 in 40 normal adults. Additionally, Kwon et al.17 examined pressure pain thresholds in 20 female patients with clinical myofascial pain syndrome and reported slightly high values of 5.4 kg/cm2 and 3.7 kg/cm2. This study examined a relatively large number of subjects (222) with pain in the musculoskeletal system of the upper limbs and reported values of 4.2 kg/cm2 and 4.5 kg/cm2, which are relatively high compared to those reported in the other papers. It appears that these differences are due to the presence or absence of musculoskeletal diseases in the subjects, the skill level of experimenters, different measurement tools, sex, dominant and non-dominant sides, and body mass index distribution.
Hogeweg et al.5 reported that a pressure algometer showed high reliability between observers for measurements of normal muscles. Some studies examined the reliability of pressure algometers in myofascial trigger points and reported high reliability between experimenters.18,19 This study also found high reliability comparable to that reported in the other studies. From these results, the examination tool was judged to be highly reliable.
In this study, no significant differences were found in all muscles examined for the comparison of pressure pain thresholds between the dominant and non-dominant sides. Other studies also reported that pressure pain threshold did not differ significantly between dominant and non-dominant sides.20,21 The results were in good agreement with those obtained in this study. This suggests that pressure pain thresholds measured between both sides show high reproducibility. In this study, most of the subjects used their right upper limbs and the measured pressure pain thresholds were significantly lower in the right side than in the left side. According to these examination results, it was expected that the pressure pain thresholds would be lower in the dominant side than in the non-dominant side. However, no difference was found in pressure pain threshold between the dominant and non-dominant sides. The reason for this is believed to be because the frequency of the non-dominant side was absolutely lower than that of the dominant side, thus failing to reflect the results of the non-dominant side. Therefore, more research is needed to reflect similar frequencies of the dominant and non-dominant sides.
Many studies have obtained different results concerning the difference in pressure pain threshold between men and women. Most of these studies reported higher pressure pain thresholds in men than in women.5,10,16 The same results were obtained in this study. The reason for the difference may be hat men tend to respond to pain more slowly than women because of the traditional social recognition that men must endure pain. The exact reason has yet to be determined. Considering the principle of pressure algometry, in which pain is induced by applying a force to a muscle and is recognized by a subject, the thicker muscle and subcutaneous tissues of men in view of anatomical characteristics may also affect the results of the studies. In actuality, men may be less susceptible to pain than women due to physiological characteristics. Further studies are required to test this hypothesis.
In this study, reliability between examiners was not analyzed because the 5 investigators did not examine the pressure pain thresholds of the same subjects. Another limitation of this study is that time-dependent analysis of reproducibility was not performed.
CONCLUSION
Digital pressure algometry showed high intra-rater reliability for PPT measurements. Diagnosis of myofascial pain syndrome based on Fischer's proposed method showed relatively high specificity and very poor sensitivity. As a result of comparing numerous research results, pressure pain threshold might be a useful parameter in assessing the effects of treatment for musculoskeletal pain and myofascial pain syndrome, taking into consideration that exact standard pressure pain thresholds of Koreans have yet to be determined. However, pressure pain threshold is not thought to be a suitable tool to diagnose or use as an early screen for myofascial pain syndrome. In addition, it is believed that the cut-off values of pressure pain threshold presented in this study will be useful as basic data for future research and clinical practice associated with pressure algometers.