INTRODUCTION
The incidence rate of hip displacement is the highest after equinus in musculoskeletal deformities in patients with cerebral palsy. If appropriate therapeutic intervention is not applied, hip displacement may develop into hip dislocation and cause postural and gait abnormalities, scoliosis, hip joint pains and problems of perineal hygiene.1,2 The subluxation or dislocation of the hip joint is one of the complications faced by children with cerebral palsy, in whom the incidence rate reaches 15% to 30% for all cerebral palsy patients. It is especially higher in patients with quadriplegic cerebral palsy.
Early therapeutic intervention is known to reduce the incidence rate of serious hip displacement in children with cerebral palsy.3 Thus, the early detection of hip displacement is critical to delay the progress of hip displacement. Various radiologic indexes have been used to detect hip displacement in children with cerebral palsy early. This is particularly true for the migration index,4 which is the most frequently used index to evaluate the risk of hip displacement and associated therapeutic effects.
In previous studies, intra-rater reliabilities were high, but inter-rater reliabilities showed different results.5-7
In most cases, the lateral edge of the acetabular roof is used as the datum point in the process where the migration index is measured. In the case of acetabular dysplasia, however, the lateral edge of the acetabular roof may be irregular in its coordinates, and therefore the measured values may be different among raters.
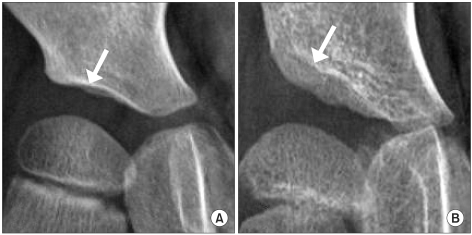
The sourcil is a shadow of dense osseous tissue that is observed at the weight-bearing surface of the acetabular roof (Fig. 1). In general, hip dysplasia can be evaluated by two methods, i.e., the classic method and the modified method. The former is to use the lateral edge of the acetabular roof as the datum point, and the latter is to use the lateral edge of the sourcil. In previous studies on the acetabular angles of patients who underwent operations for developmental hip displacement, it was reported that the modified method was more useful to evaluate hip dysplasia.8-10
Also in children with cerebral palsy, the measured value may be different according to datum points. Nevertheless, there has been no comparative study on the classic method and the modified method in relation to the migration index. This study analyzed intra-rater and inter-rater reliability not only in the classic method but in the modified method, as well as to study the clinical significance.
MATERIALS AND METHODS
Subjects
This study was conducted on patients with cerebral palsy who visited the rehabilitation department at this hospital and underwent plain radiographies on their hip joints (200 hip joints) between August 2009 and December 2009. The study group consisted of 66 boys and 34 girls, whose average age was 7.88±1.54 years.
Methods
Subjects were assisted to take a supine position so their their pelvises could be parallel to each other and both their coxae could be in a neutral position while undergoing plain hip radiographies.11,12 This study was retrospectively conducted, and hip displacement was measured by two raters (A and B) using plain hip radiographs. The two raters were well-acquainted with pelvic and coxal structures and radiologic indexes, and measured hip displacement in accordance with standardized methods.4
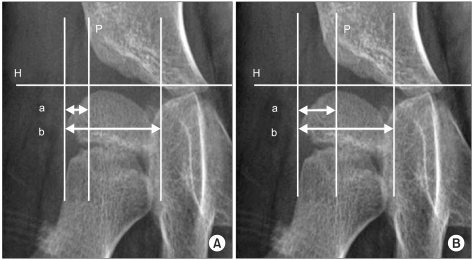
The outermost edge of the acetabular roof was regarded as the datum point from where the Perkin's line (P-line) was drawn. Likewise, another P-line was drawn from the lateral edge of the sourcil. The former and the latter method were defined as the classic and modified method, respectively (Fig. 2).
To evaluate intra-rater reliability, the displacement of 200 hip joints was measured 3 times at intervals of 1 week without data on previous measurements, and an analysis was made of the reliability amongst measured values. In order to evaluate inter-rater reliability, the displacement of 200 hip joints was measured in the same way, and an analysis was made of the reliability amongst mean values.
The reliabilities were evaluated in patients with or without hip dysplasia. In accordance with the descriptions of Ogata et al.13 and Agus et al.,8 the acetabular roof was classified as to the shape of the sourcil. Type I and II cases where the lateral edge of the acetabular roof and that of the sourcil are superimposed, were regarded as normal. On the other hand, type III and IV were classified as hip dysplasia.
Statistical analysis
Intra-rater reliability and inter-rater reliability were evaluated by use of Intraclass Correlation Coefficient (ICC), and the standard error of measurement (SEM) was calculated on the basis of inter-value differences and standard deviation. The data were analyzed by use of the program SPSS 18.0.
RESULTS
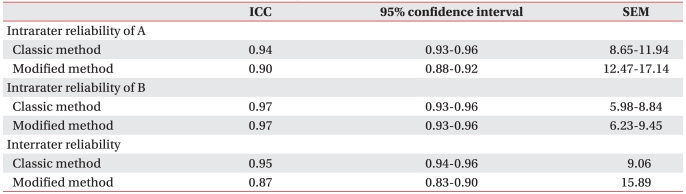
Intra-rater reliability was within reliable levels for both raters. In the case of rater-A, ICC indicated 0.94 and 0.90 in the classic method and the modified method, respectively. SEM indicated 8.64 to 11.94 and 12.48 to 17.14 respectively. In the case of rater-B, ICC was 0.97 in both methods. SEM indicated 5.98 to 8.84 and 6.23 to 9.45, respectively, and thus the error range was narrower in the classic method (Table 1).
In the case of Inter-rater reliability, ICC indicated 0.95 and 0.87 in the classic method and the modified method, respectively. SEM indicated 9.06 and 15.89, respectively, and thus was higher in the classic method (Table 1).
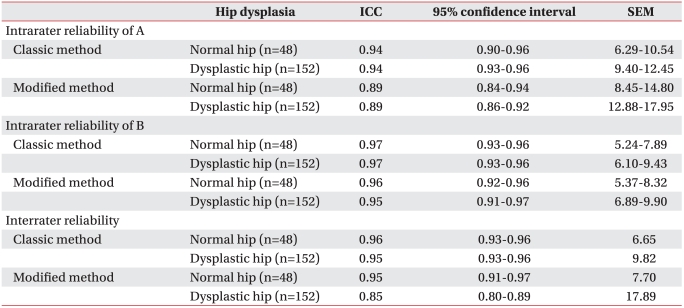
Intra-rater reliability was evaluated in both methods and groups. In the case of rater-A, ICC indicated 0.94 and 0.89 in the classic method and the modified method, respectively, irrespective of group. On the other hand, SEM indicated 8.45 to 14.80 and 12.88 to 17.95 in the normal group and the dysplasia group, respectively, and was thus lower in the normal group. In the case of rater-B, ICC in the classic method indicated 0.97 irrespective of group. In the modified method, it indicated 0.96 and 0.95 in the normal group and the dysplasia group, respectively. SEM was lower in the normal group, which was similar to that of rater-A (Table 2).
Inter-rater reliability was evaluated in both methods and in both groups. In the case of the classic method, ICC indicated 0.96 (SEM: 6.65) and 0.95 (SEM: 9.82) in the normal group and the dysplasia group respectively, and thus it was higher in the normal group. In the case of the modified method, it indicated 0.95 (SEM: 7.70) and 0.85 (SEM: 17.89) respectively. Likewise, it was higher in the normal group (Table 2).
DISCUSSION
The subluxation or dislocation of the hip joint can be conveniently identified by frontal-view radiographs. For this, various indexes including the migration index, the acetabular index and center-edge angle are widely used. The selection of such indexes should be based on the patient's age or disease. The migration index is to show how much the ossified femoral head has been dislocated from the ossified acetabular roof, which is widely used in children with cerebral palsy who have open triradiate cartilages.4,14
The integration index can be easily measured, and its SEM is within ±10%. It can be easily applied to a broad age range and thus may be the most useful index to check for subluxation of the hip joint in children with cerebral palsy.4 In many studies, follow-ups were conducted on migration indexes for several months, and as a result the significant progress of hip dysplasia was defined as where SEM was over 10%. In addition, these studies reported that the migration index was useful to evaluate the effects of therapeutic interventions, such as selective dorsal rhizotomy, hip abductors and soft tissue surgery, in the subluxation of the hip joint.15-20
A follow-up on the migration index involves the proof of a decrease or increase in hip dysplasia. In this regard, it is imperative to secure intra-rater and inter-rater reliabilities. In the study conducted by Parrott et al.5 in 2002, 20 hip joints were measured 2 times by 2 raters. Inter-rater and intra-rater reliabilities were high in that ICC was over 0.9. SEM indicated ±8.3% in relation to intra-rater reliability. This suggests that when hip migration occurred, SEM reached over 8.3% when one rater conducted a follow-up. In the study conducted by Pountney et al.6 in 2003, 40 hip joints were measured 3 times by 3 raters. SEM indicated ±7.6% and ±8.1% in relation to intra-rater reliability and inter-rater reliability respectively, which implies that the reliability was clinically reliable like previous studies.
In the study of Faraj et al.7 conducted on 44 hip joints of patients with cerebral palsy (2004), intra-rater reliability was not over 13% (95% confidence interval) but inter-rater reliability reached 21 to 23%, and thus the results were inapplicable clinically. They maintained that the migration index should be measured by one rater.
Error is caused by measurement variability, inaccurate measurements or inaccurate records. In particular, the accurate determination of the datum point is critical for measurement of the migration index.6 Nevertheless, the datum point was specified only in the study of Parrott et al.5
In this study, the datum point was specified with the classic method and the modified method, whereas intra-rater and inter-rater reliabilities showed high levels with the ICC of over 0.9, which shows that the accurate determination of the datum point raises the reliability.
In relation to intra-rater reliability, SEM was lower in the classic method than in the modified method, which was similar to the results of previous studies.
In the normal hip joint, the sourcil is evenly thick and semicircular. Its lateral part is horizontal or downwardly.9,10 In case the sourcil inclines upward or is irregular in thickness, it applies uneven stress to the hip joint. Thus, the correct form of sourcil may be a criterion for acetabular dysplasia (Fig. 1). In 2000, Kim et al.11 reported that the inter-rater error may be reduced when the lateral edge of the sourcil was used as the datum point for the measurements of the migration index and the center-edge angle. In addition, they studied the anatomic structure of the sourcil by use of MRI, 3D CT and arthrographies. According to the results, the lateral edge of the sourcil fell under the lateral center of the acetabular roof. However, on radiographs the shadow of the lateral bone meant the anterolateral edge of the acetabular roof, i.e., the inferior region of the anterior inferior iliac spine.
In previous studies, it was reported that the modified method may effectively distinguish dysplastic hip joints from normal ones.8,13 However, in this study it was found that the modified method was inferior to the classic method in intra-rater and inter-rater reliabilities. As the case stands, the modified method is likely to produce unreliable results if the migration index is measured by different raters or in cases of severe hip dysplasia.
CONCLUSION
This study was conducted to compare the classic and modified method in reliability, with children that had cerebral palsy. As mentioned, the former is to use the lateral edge of the acetabular roof as the datum point, and the latter is to use the lateral edge of the sourcil. The results showed that the lateral edge of the acetabular roof was a more effective datum point than that of the sourcil, in terms of reliability. Particularly in relation to hip dysplasia, the lateral edge of the acetabular roof was found to be more reliable as the datum point than that of the sourcil. This proves how important the datum point is in measuring the migration index of children with cerebral palsy. In conclusion, the lateral edge of the acetabular roof may be more effective than that of the sourcil.