INTRODUCTION
Oropharyngeal dysphagia is a common and clinically relevant symptom in patients with parkinsonism [1]. Parkinsonism can be classified into primary and secondary phases. In primary cases, it is subclassified into idiopathic ParkinsonвҖҷs disease (IPD) and atypical parkinsonism [2]. Dysphagia in the on-state condition was documented in 68% of patients with late-stage ParkinsonвҖҷs disease (PD) [3]. In addition, swallowing dysfunction was observed in more than 50% of subjectively asymptomatic patients with PD [4]. The prevalence of oropharyngeal dysphagia based on subjective outcomes in patients with PD is 35%, which increases to 82% considering objective measures of swallowing dysfunction [5]. Patients with atypical parkinsonism, such as those with progressive supranuclear palsy, multiple system atrophy, and corticobasal degeneration, are known to develop dysphagia earlier than those with IPD [6].
Dysphagia related to parkinsonism is known to be affected by both central and peripheral nervous system mechanisms [7-9]. These pathological changes eventually lead to clinical complications such as insufficient medication intake, malnutrition, dehydration, and aspiration pneumonia which is known to greatly affect mortality [10]. Therefore, it is essential to evaluate and manage the risk of respiratory infections in patients with parkinsonism and dysphagia.
Our previous studies using a nationwide database demonstrated that patients with PD had a 2.23-fold higher risk of pneumonia and a 4.21-fold higher risk of aspiration pneumonia than non-PD controls [11,12]. We also reported significant risk factors for respiratory infections such as old age, male sex, region of residence, and several comorbidities. Similar results were reported in a nationwide population-based study conducted in another country [13]. However, these previous studies only identified general risk factors for respiratory infection which were not specific to parkinsonism, and they did not provide information on the characteristics of dysphagia in their study population.
Videofluoroscopic swallowing studies (VFSS) are the gold standard for evaluating swallowing and confirming dysphagia and are widely used in recognition of their reliability [14]. Several studies have reported abnormal swallowing features using VFSS in patients with parkinsonism [15-17]. However, few studies have investigated the relationship between dysphagia and respiratory infections in these patients. In patients with neurodegenerative diseases, such as PD and dementia, who underwent aspiration during thin-liquid swallowing by VFSS, liquid thickening showed no superiority in the prevention of pneumonia and caused a higher incidence of dehydration, urinary tract infection, and fever than the chindown posture without liquid thickening in a large randomized trial [18]. Therefore, the clinical and swallowing characteristics and the risk of respiratory infection should be carefully considered for the proper management of dysphagia in patients with parkinsonism. A recent study suggested that mastication, lingual motility prior to transfer, aspiration, and total shallow time are significant prognostic factors in patients with PD with aspiration pneumonia [19]. Current research on prognostic factors of respiratory infection in patients with parkinsonism is insufficient. Therefore, additional research is required to clarify these factors thoroughly.
This study aimed to investigate the clinical and swallowing characteristics related to a history of respiratory infection in patients with parkinsonism based on the hypothesis that certain clinical features and swallowing patterns identified through VFSS are associated with the risk of respiratory infection.
MATERIALS AND METHODS
Participants
Patients with parkinsonism who were referred for VFSS because of dysphagia symptoms from December 2015 to November 2018 were retrospectively assessed for eligibility in this study. The inclusion criteria were: (1) history of VFSS to evaluate swallowing function; (2) primary parkinsonism, IPD, or atypical parkinsonism as the cause of dysphagia; and (3) age 19 years or older at the time of VFSS. In this study, the diagnostic criteria for IPD were based on the UK ParkinsonвҖҷs Disease Society Brain Bank criteria [20], while atypical parkinsonism subtypes were diagnosed according to their specific clinical features and respective diagnostic criteria, such as multiple system atrophy [21], progressive supranuclear palsy [22], and dementia with Lewy bodies [23]. The exclusion criteria were: (1) ongoing diet with tube feeding or parenteral nutrition only; (2) other diseases that may affect dysphagia, such as stroke, traumatic brain injury, myopathies, and head and neck cancers; (3) secondary parkinsonism, such as vascular parkinsonism and drug-induced parkinsonism; and (4) insufficient medical records.
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB No. H-2111-179-1277). The requirement for informed consent was waived owing to the retrospective nature of the study.
Data acquisition
Demographic and clinical characteristics and initial VFSS findings were evaluated using the Videofluoroscopic Dysphagia Scale (VDS) and scores from the Korean Version of the Swallowing Disturbance Questionnaire (KSDQ) were collected from patientsвҖҷ medical records [24]. Clinical characteristics included age, sex, diagnosis, onset of parkinsonism and dysphagia, current diet type, previously recommended diet, antiparkinsonian medications, and Hoehn and Yahr (H&Y) stage at the time of VFSS for disease severity. Medication use at the time of the VFSS was roughly evaluated by calculating the levodopa equivalent dose (LED) [25]. The diagnosis was classified as either IPD or atypical parkinsonism, including multiple system atrophy, progressive supranuclear palsy, corticobasal degeneration, and dementia with Lewy bodies. Patients whose parkinsonism type was undetermined until study registration were classified as вҖңnot defined.вҖқ
Swallowing evaluation was performed at 30 frames per second through digital videofluoroscopy. All patients underwent VFSS while maintaining their regular medication regimen on the test day. The study was performed by two physiatrists using the revised protocol of the Logemann study [26,27]. Formal reading was based on the agreement of physiatrists with expertise in swallowing dysfunction. To evaluate the functional analysis of swallowing using VFSS as an objective quantitative score we used the VDS. VFSS findings consisted of 14 VDS subdomains [28], including lip closure, bolus formation, mastication, apraxia, tongue-to-palate contact, premature bolus loss, oral transit time, triggering of pharyngeal swallow, vallecular residue, laryngeal elevation, pyriform sinus residue, coating of the pharyngeal wall, pharyngeal transit time, and aspiration.
The SDQ is a self-report questionnaire used to detect swallowing problems in patients with PD [29]. In addition, it has been reported to be a sensitive and accurate tool for identifying dysphagia arising from various etiologies [30]. The SDQ consists of 15 questions and the last question asks for a history of respiratory infections, such as pneumonia or bronchitis, in the past year. In this study, the score for the last question was used to divide the patients into those with and without a history of respiratory infection. K-SDQ data was collected from the patient on the day of VFSS examination.
Statistical analysis
Clinical characteristics and VFSS findings were compared between patients with and without a history of respiratory infection in the past year. With regards to the demographic and clinical characteristics, age was found to be normally distributed and was analyzed using a StudentвҖҷs t-test. For disease duration, dysphagia duration, and LED, a MannвҖ“Whitney U-test was performed as they did not meet the normality assumption. Other items were analyzed using FisherвҖҷs Exact Test. Among the VFSS items, premature bolus loss, vallecular and pyriform sinus reserve, and aspiration were analyzed using the MannвҖ“Whitney U-test, while other VDS items were analyzed using FisherвҖҷs Exact Test. The chi-square test was used for sex, diagnosis (IPD vs. atypical parkinsonism), and H&Y stage (stage IвҖ“III vs. stage IVвҖ“V). Regarding VFSS findings, the MannвҖ“Whitney U-test was used for premature bolus loss, vallecular, and pyriform sinus residues, and aspiration. FisherвҖҷs exact test was used for other VFSS findings. We used the IBM SPSS version 26.0 (IBM Corp., Armonk, NY, USA) for statistical analysis, and statistical significance was defined as p<0.05.
Furthermore, a multivariate logistic regression model was used to identify the clinical and swallowing characteristics related to history of respiratory infection. We created a model for each clinical characteristic and VFSS finding. Variables in the univariate analysis (p<0.05) were selected and entered into the model, and forward selection was used as the variable selection method.
RESULTS
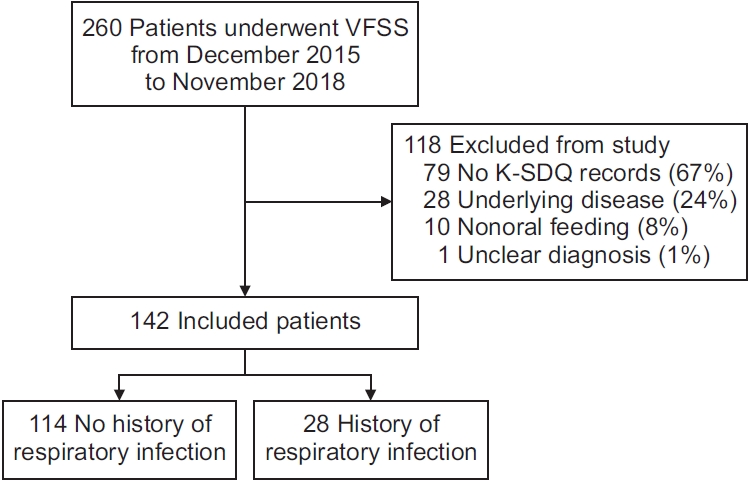
Of the 260 patients identified with parkinsonism who underwent VFSS from December 2015 to November 2018, 142 were included in this study (Fig. 1). The reasons for the 118 exclusions were no K-SDQ records (n=79, 67%), underlying diseases (n=28, 24%), nonoral feeding (n=10, 8%), and unclear diagnosis (n=1, 1%). Of the 142 patients, 28 had a history of respiratory infection.
The demographic and clinical characteristics of patients are shown in Table 1. The mean patient age was 71.50Вұ9.22 years, 84 (59.2%) were male, the mean disease duration was 6.50Вұ4.78 years, and the mean duration of dysphagia was 1.63Вұ1.97 years. Sixty-six (46.5%) patients had a diagnosis of IPD. Patients with respiratory infections were older (74.75Вұ10.20 vs. 70.70Вұ8.83, p=0.037), had a higher H&Y stage (stage IVвҖ“V, 67.9% vs. 49.1%; p=0.047), and were more likely to have a diagnosis of IPD (67.9% vs. 41.2%, p=0.011) than those without.
Differences in VFSS findings between patients with and without a history of respiratory infection are presented in Table 2. Abnormal findings in bolus formation (85.7% vs. 61.4%, p=0.015), premature bolus loss (67.9% vs. 56.1%, p=0.025), oral transit time (28.6% vs. 11.4%, p=0.035), pyriform sinus residue (64.3% vs. 39.5%, p=0.010), pharyngeal wall coatings (67.9% vs. 43.9%, p=0.034), and aspiration (96.4% vs. 86.8%, p=0.027) were significantly more frequent in patients with respiratory infections than in those without.
Regarding clinical characteristics, H&Y stage (stage IвҖ“ III vs. stage IVвҖ“V; odds ratio [OR], 3.174; 95% confidence interval [CI], 1.226вҖ“8.216; p=0.017) and diagnosis of IPD (atypical parkinsonism vs. IPD; OR, 0.280; 95% CI, 0.111вҖ“0.706; p=0.007) were significantly related with respiratory infection in the multivariate analysis (Table 3). Regarding VFSS findings, pyriform sinus residue (>50% vs. none; OR, 14.615; 95% CI, 2.257вҖ“94.623; p=0.005) and premature bolus loss (>50% vs. none; OR, 5.151; 95% CI, 1.047вҖ“25.338; p=0.044) were also significantly associated with respiratory infection in the multivariate analysis (Table 4).
DISCUSSION
This study aimed to investigate clinical and swallowing characteristics related to a history of respiratory infections in patients with parkinsonism. In this study, clinical characteristics, including diagnosis and disease severity, and VFSS findings, including pyriform sinus residue and premature bolus loss, were associated with respiratory infections. Prolonged oral transit time showed a borderline significance in the multivariate analysis (OR, 2.672; 95% CI, 0.854вҖ“8.364; p=0.091). An intriguing finding might be that oral phase-related abnormalities are risk factors for respiratory infection in this population. In addition, unlike previous studies, this study is more robust because both clinical and swallowing characteristics were considered to reveal risk factors for respiratory infection in patients with parkinsonism, although separate models were developed for each characteristic owing to the limited study population.
H&Y stage and diagnosis were significant risk factors for respiratory infection in the multivariate logistic regression model for clinical characteristics. In this model, patients with a greater disease severity showed an approximately three-fold higher risk of respiratory infection than those in mild to moderate disease stages. Our results are in line with previous findings that subjective and objective dysphagia are correlated with disease severity [5], and respiratory infection is a major cause of death in patients with PD [31,32]. Patients with IPD showed a higher risk of developing respiratory infection than those with atypical parkinsonism. This result should be interpreted cautiously because the present study was a crosssectional study of patients with parkinsonism who underwent VFSS because of dysphagia symptoms or signs. It is well known that dysphagia appears earlier in patients with atypical parkinsonism than in patients with PD [1]. The median latencies of dysphagia have been reported to be 42вҖ“67 months in patients with atypical parkinsonism and 130 months in those with PD [33]. The average disease duration in our study population was 3.93 years, 3.95 years, and 8.21 years in patients with multiple system atrophy, progressive supranuclear palsy, and IPD, respectively. Therefore, it is necessary to comprehensively consider the characteristics of each diagnosis when evaluating the risk of respiratory infection in patients with parkinsonism after VFSS.
In the present multivariate regression model, premature bolus loss and pyriform sinus residue were significant risk factors for respiratory infection, and oral transit time was also borderline significant. Previous studies comparing VFSS findings in patients with PD and controls have shown that pyriform sinus residue may be associated with respiratory infections [34]. Premature bolus loss, which may cause pre-swallow aspiration, is also a typical finding in dysphagia in PD [35]. In addition, hypokinesia and bradykinesia cause decreased motor function of the tongue and delayed oral transit time in PD [36,37]. Therefore, oral phase-related abnormalities could have a great impact on the risk of respiratory infection in patients with parkinsonism. A recent study also reported that lingual motility and swallow time are significant prognostic factors for aspiration pneumonia in patients with PD [19].
Aspiration was a significant factor in the univariate analysis, but it was excluded in the final multivariate analysis model. One of the possible reasons may be that our study investigated factors associated with respiratory infection as a broader category, while the previous study focused specifically on aspiration pneumonia [19]. In addition, it has been reported that the likelihood of developing pneumonia was low in PD patients with liquid aspiration, regardless of liquid thickening [18]. Chronic dysphagia in slowly progressing degenerative diseases is presumed to have distinct characteristics from acute dysphagia, such as that caused by a stroke. Therefore, factors such as disease progression and oral function play a more significant role in PD and require different approaches for managing dysphagia.
Although the following factors were not selected in the final model of our study, several previous studies have reported that older age, male sex, and aspiration shown in VFSS are common risk factors for respiratory infection [11-13]. In our study, age was significant in the univariate analysis but not in the multivariate model. The interaction between age, disease severity, and diagnosis may affect our results since disease severity usually increases with age, and the age of disease onset varies depending on the type of parkinsonism. The statistical power which was limited by the number of participants may also affect the results. Previous studies have also shown that many comorbidities increase the risk of pneumonia in patients with PD [11-13]. Although underlying medical conditions were not included in the present study, major comorbidities known to increase the risk of pneumonia, such as chronic heart disease, chronic kidney disease, and dementia, should be considered together.
This study had several limitations. First, although our study included 142 participants, only two to three factors could be input in the model because only 28 participants had a history of respiratory infection. A lack of statistical power may lead to a type 2 error, but our results suggest several significant risk factors for respiratory infection in patients with PD, some of which were not covered in previous studies. Second, the presentation of respiratory infections was identified using a questionnaire. As this relies on the patientвҖҷs memory, its diagnostic accuracy could be limited. Finally, because this was a retrospective study, there could be other potential confounders and inaccurate records. The VFSS test was conducted while the patient was taking their regular medication. However, the time elapsed between drug administration and the VFSS test was not recorded. This makes it challenging to determine the on/off medication state of the patient, which is a further limitation of the retrospective nature of the study. The impact of levodopa on the swallowing function in PD patients has been a subject of debate. A recent review has suggested that levodopa might improve swallowing efficiency without effect on swallowing safety in PD patients [38]. Therefore, our findings should be verified prospectively in future studies.
In conclusion, this study suggests that disease severity, diagnosis, pyriform sinus residue, and premature bolus loss observed in VFSS are associated with respiratory infection in patients with parkinsonism. These characteristics should be considered when evaluating the risk of respiratory infection in patients with dysphagia with parkinsonism. Further prospective studies are required to validate our results.