INTRODUCTION
Adhesive capsulitis (AC), often referred to as frozen shoulder, is one of the most common causes of upper-extremity pain. Its etiology includes various diseases, such as long-term immobilization, advanced age, surgical treatment, trauma, diabetes mellitus, herniated disc, and stroke [1]. Synovial inflammation and subsequent reactive capsular fibrosis of the glenohumeral joint capsule are known pathophysiological mechanisms of AC [2,3].
Physical therapy, anti-inflammatory drugs, oral steroids, hydrodilatation (HD), and intra-articular corticosteroid injections are common treatments for AC [4]. Combining HD with corticosteroid therapy, in which steroids and a sufficient amount of isotonic sodium chloride solution are injected into the glenohumeral joint capsule, has been reported to improve the range of motion (ROM) of the shoulder and reduce pain and inflammation [5,6]. As a result, HD with corticosteroid injection is one of the treatment regimens often used in patients with AC.
AC is a common complication of breast cancer surgery, especially in patients who undergo axillary lymph node dissection [7–9]. Despite advances in less invasive and more selective surgical procedures for breast cancer, many disorders causing upper-extremity dysfunction and pain, such as AC, occur even after surgery [7,10]. Previous studies have reported that the prevalence of AC between 13 and 18 months post-breast cancer surgery was 10.3% [11] and increased to 22.2% until 5 years after surgery in Asian patients with breast cancer [12].
Although the exact pathophysiology of AC after breast cancer surgery is unknown, it may be affected by the surgery itself, postoperative shoulder movement restrictions, lymphedema, and radiation therapy [7]. However, since it is conventionally accepted that there is no fundamental difference from other mechanisms, the treatment method proceeds in the same manner as idiopathic AC [8].
To our knowledge, no published research has reported whether HD with corticosteroid injection has an effect on AC after breast cancer surgery or whether the pathological condition is similar to idiopathic AC. Advances in real-time pressure–volume monitoring techniques for HD have provided information on the biomechanical properties of the glenohumeral joint capsules related to AC [13,14] and hemiplegic shoulder pain [15].
This study aimed to evaluate the effects of HD with corticosteroid injection on the passive ROM and pain and disability scores of the shoulder affected with AC after breast cancer surgery and identify the biomechanical properties of the glenohumeral joint capsule.
MATERIALS AND METHODS
Breast cancer surgery group (BC group)
A total of 24 consecutive patients were prospectively enrolled in this study (Fig. 1). The enrolled patients were diagnosed with AC after breast cancer surgery and scheduled for HD. The Institutional Review Board of Seoul National University Hospital approved this study (No. 1606-137-774), and all participants provided written informed consent in conformance with the ethical standards of the Declaration of Helsinki.
AC was defined as an insidious painful condition with limited shoulder ROM in at least two directions. The limited ROM in each direction of the shoulder was <30° for external rotation, <130° for flexion, and <80° for abduction on goniometric measurements [13,15]. Patients were excluded when they had any systemic or structural disorders that could result in limited ROM or pain, such as major trauma, shoulder surgical history, rotator cuff tear, or inflammatory joint disease. Male patients and patients with stage IV breast cancer were also excluded. The sample size was determined via consultation with the Medical Research Collaborating Center at the hospital.
Idiopathic AC group (CON group)
The CON group consisted of patients who were diagnosed with AC and received HD for the first time (Fig. 1). This group had the same inclusion and exclusion criteria as the BC group but did not include any patients with breast cancer. The participants in the CON group completed baseline clinical and biomechanical assessments on their first visit, and their data were analyzed with no additional follow-up.
ROM and SPADI in the BC group
Clinical and sonographic evaluations were performed to assess patient eligibility prior to HD. Passive shoulder ROM was measured using a long-arm goniometer while the patients were sitting on a stool. Shoulder abduction was assessed in the coronal plane, with the shoulder externally rotated. Forward flexion was measured in the sagittal plane, with the hands pronated. External rotation was measured in the transverse plane, with the shoulder adducted and the elbow flexed at 90° [16]. The measured ranges of abduction, flexion, and external rotation were summed and used for the analysis of treatment progress [17].
The Shoulder Pain and Disability Index (SPADI) is a self-report questionnaire that can be administered in an outpatient setting and has been used in many patients with shoulder diseases, including AC [18]. It consists of 13 questions in two domains: pain (five items) and disability (eight items) to evaluate shoulder pathology-related pain and disability. Each question is scored on a visual analog scale ranging from 0 to 10, where 0 indicates no difficulty/no pain and 10 indicates most difficult/worst pain. Each item in both domains is assigned the same weight and eventually changed to a score ranging from 0 to 100. Herein, the prospective participants underwent baseline ROM assessment, clinical survey (SPADI), ultrasonography, and HD-related biomechanical assessment on their first visit and follow-up ROM assessment and clinical survey (SPADI) at 2 and 4 weeks after the procedure.
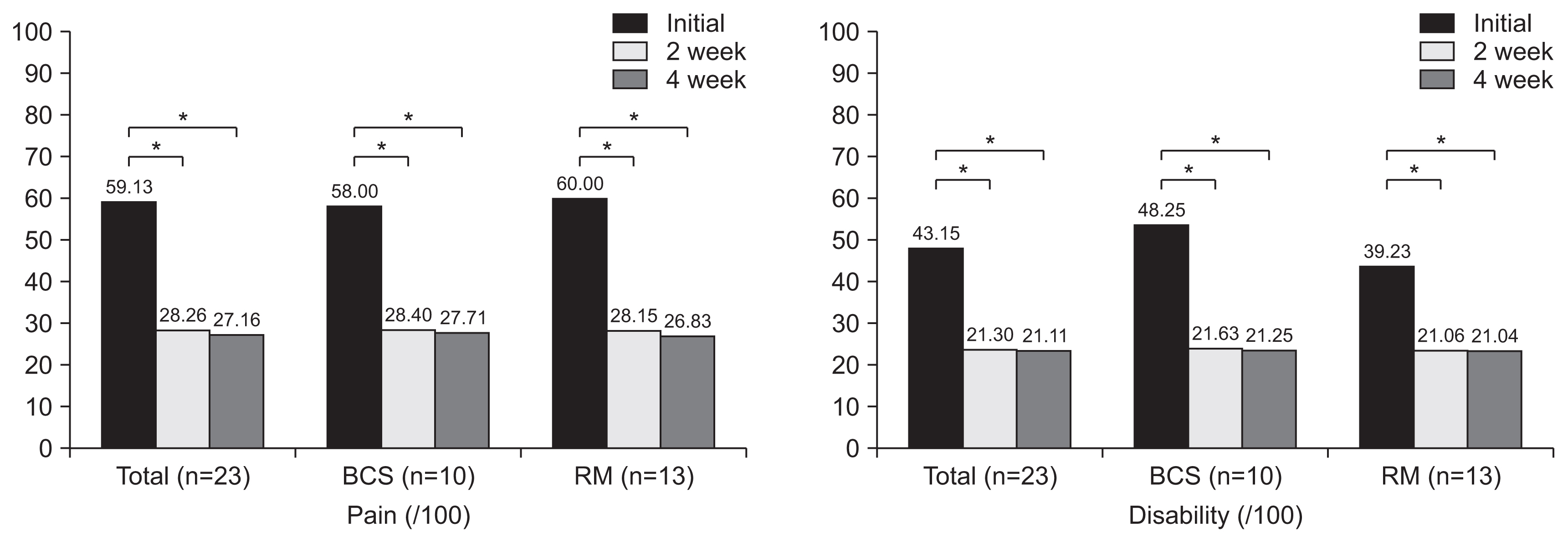
The BC group was further subdivided into breast-conserving surgery (BCS) and radical mastectomy (RM) groups according to the surgical method, and the difference between these subgroups was evaluated.
Biomechanical properties of the BC and CON groups
Intra-articular HD of the shoulder to evaluate the biomechanical properties of the glenohumeral joint capsules was performed following the standard protocol reported in previous studies [13–15]. Initially, the participants sat on a chair with a pronated forearm on the thigh. They were asked to remain sufficiently relaxed to avoid changing the intra-articular pressure of the affected shoulder. After skin disinfection, a 22-gauge spinal needle was inserted into the posterior intra-articular space under ultrasound guidance (Accuvix V20; Medison, Seoul, Korea) and then connected to the pressure-monitored HD system. This machine is designed for constant volume–speed fluid infusion and simultaneous intra-articular pressure monitoring [13–15]. The injectate consisted of a total of 50 mL mixture including 1 mL (40 mg) triamcinolone, 10 mL 1% lidocaine, and 39 mL isotonic sodium chloride solution. The fluid was infused at a rate of 7 mL per minute. When the examiner observed that the pressure was too high or the participants felt much pain, the infusion was stopped temporarily until the intra-articular pressure and pain stabilized. The fluid infusion was terminated when the intra-articular pressure increased to 800 mmHg, the pressure–volume profiles reached the third phase, or the patients requested to terminate the procedure because of excessive pain or discomfort. This procedure generated typical pressure–time curves. One patient in the BC group (n=24) and one patient in the CON group (n=45) stopped the procedure because of severe pain and vasovagal symptoms, respectively (Fig. 1).
Because the fluid was injected at a constant rate (7 mL per minute), it was easy to convert to a pressure–time curve. The pressure–time curve generally consists of three phases: initial filling phase (first), elastic deformation phase (second), and plastic deformation phase (third). The slope of the second phase is thought to be caused by stiffness of the shoulder joint capsule (Scap). The capsular pressure at the maximal volume (Pmax) and capsular capacity (Vmax, total infused volume) were also recorded as biomechanical parameters of the shoulder joint capsules [14] (Fig. 2).
All patients received brochures on shoulder home exercises for AC and were educated on stretching exercises once before HD [19]. They were instructed to continue their daily home exercises after the procedure.
Statistical analysis
All statistical analyses were performed using the SPSS software version 26.0 (IBM, Armonk, NY, USA). We compared the demographic factors (age, height, weight, duration of symptoms, involved side, diabetes mellitus, and surgical method) and biomechanical parameters (Vmax, Pmax, and Scap) between the two groups using an independent t-test or the Mann-Whitney test, depending on normal distribution satisfaction. Within-group analysis was performed using paired t-tests when the difference between the baseline and follow-up test results was normally distributed. The Wilcoxon signed-rank test was performed when the results were not normally distributed. Statistical significance was defined as a p-value of <0.05.
We also compared the SPADI score (pain sub-score, disability sub-score, and total score) and ROM (flexion, abduction, external rotation, and total ROM) before HD and at 2 and 4 weeks after the procedure in the BC group. For the three timelines, analysis of variance or the Kruskal-Wallis test (when the assumptions of parametric statistical analysis were not satisfied) was used. The values that differed between the three points were analyzed using Bonferroni correction, and statistical significance was defined as a p-value of <0.017.
RESULTS
Demographic characteristics of the BC and CON groups
There were no significant differences between the two groups, except for age. The mean patient age was 51.30±6.58 years in the BC group and 57.38±8.63 years in the CON group (p=0.005). The mean height was 158.67±5.10 cm in the BC group and 158.69±7.43 cm in the CON group (p=0.986). The mean weight was 56.87±5.29 kg in the BC group and 59.76±8.75 kg in the CON group. The mean duration of symptoms was 7.63±5.51 months in the BC group and 11.26±12.24 months in the CON group. The right side was involved in 15 patients (65.2%) in the BC group and 34 patients (80.9%) in the CON group. Four patients (17.4%) in the BC group and six patients (14.3%) in the CON group had diabetes mellitus. In the BC group, 10 (43.5%) and 13 (56.5%) patients underwent BCS and RM, respectively (Table 1).
Biomechanical properties of the BC and CON groups
Among the biomechanical parameters, the Pmax and Scap were significantly different between the two groups (Table 2). The Pmax (519.67±120.90 vs. 424.78±104.42 mmHg; p=0.002) and Scap (19.69±10.58 vs. 11.55±7.77 mmHg/mL; p=0.001) were significantly higher in the BC group than in the CON group. There was no significant difference in the Vmax between the two groups. All three biomechanical features showed no significant difference between the BCS and RM subgroups divided according to the type of surgery within the prospective BC group (Table 2).
Changes in the ROM and SPADI disability and impairment scores in the BC group
Significant changes were observed in the post-treatment ROM and SPADI scores. All ROM (abduction, flexion, external rotation, and total ROM) and SPADI scores (pain, disability, and total score) significantly improved (Table 3, Fig. 3). The total ROM was 214.67°±48.48° before HD and 286.23°±50.98° and 311.87°±37.74° at 2 and 4 weeks after HD, respectively. As shown in Table 3, the greatest improvement in all ROM was observed between the initial and post-2-week evaluations (p<0.017). Although the mean ROM increased between weeks 2 and 4, the difference was not significant.
In the BC group, both BCS and RM subgroups showed significant improvements in all ROM and SPADI scores at 2 and 4 weeks after HD compared with the baseline values. In the within-group analysis of the effect of the shoulder ROM, both subgroups showed significant improvements at 2 and 4 weeks after HD. However, there was no significant difference in any of the ROM between 2 and 4 weeks after HD. In the comparison of the shoulder ROM changes between the BCS and RM subgroups, no significant difference was identified in all ROM at baseline and 2 weeks after HD. However, at 4 weeks post-HD, the ranges of shoulder flexion and external rotation and total ROM in the BCS group were significantly greater than those in the RM group (Table 3).
Significant results were also observed in the SPADI score changes. After the intervention, there was a significant decrease in both pain and disability sub-scores, as shown in Fig. 3 (p<0.001). Twenty-one patients (91.3%) presented with decreased pain and disability sub-scores; however, there was no improvement or slight deterioration in two patients. The greatest improvement in all SPADI scores was seen between the initial and 2-week follow-up evaluations, and no significant differences were found between the 2- and 4-week follow-up evaluations, similar to the ROM results (Table 3, Fig. 3).
Although the within-group changes confirmed significant improvements in both pain and disability sub-scores after the intervention, no significant change between the 2- and 4-week post-HD evaluations was observed. The pain and disability sub-scores and total SPADI score did not significantly differ between the subgroups (Fig. 3, Table 3).
DISCUSSION
This study examined the effects of HD with corticosteroid injection on the passive shoulder ROM and SPADI pain and disability sub-scores in patients with AC after breast cancer surgery. During this study, all 23 patients showed improvements in the shoulder ROM, and most of them (91.3%) showed an improvement in pain and disability. Several previous studies have reported improvements in the ROM after intra-articular injection in patients with idiopathic AC [20–22]. In a recent study, HD with corticosteroid injection was suggested to be more effective in relieving pain and improving limited ROM for frozen shoulder than intra-articular or subacromial steroid injection [23]. In addition to the effect of corticosteroids, HD is thought to be responsible for treating AC through extrinsic and intrinsic factors [24]. The mechanical effect of capsular distention through a large injection volume causes the release of the joint by expanding the volume capacity and decreasing the tendency of intra-articular pressure [17]. Another intrinsic mechanism of joint distention is that it reduces the condition of increased glycosaminoglycan concentration and myofibroblast activity in patients with AC [25]. Piotte et al. [20] reported that the passive shoulder ROM improved by 18.6° for abduction, 17.2° for flexion, and 24.4° for external rotation 3 weeks after the first HD. In our study, the ROM at 2 weeks after HD changed by 26.26° for abduction, 23.83° for flexion, and 21.48° for external rotation, with statistical significance. In addition, the average ROM changes between the baseline and 2-week follow-up evaluations and between the 2- and 4-week follow-up evaluations were calculated as 32.56° for abduction, 28.16° for flexion, and 23.65° for external rotation. The range of external rotation improved to a similar extent; however, the ranges of abduction and flexion showed greater improvements herein than in the study by Piotte et al. [20]. Although a direct comparison was difficult because of the differentiation between the ROM measurement methods (e.g., patient position) and the HD procedure technique, our study suggests that the effects of HD with corticosteroid injection on ROM improvement in patients with AC after breast cancer surgery are similar to or greater than the effects on ROM improvement in patients with idiopathic AC.
Obvious improvements in the ROM were observed in the first 2 weeks after treatment. The patients were instructed to perform home exercise programs for 4 weeks; however, there was no significant improvement in the ROM between the 2- and 4-week follow-up evaluations. In an earlier study, intra-articular corticosteroid injection was more effective in improving shoulder disability and pain in patients with AC than supervised physiotherapy [26]. Another study stated that physiotherapy following joint distension had a positive effect on the active ROM of the shoulder, but yielded no effect on the pain, function, and quality of life (QOL) of patients with AC [27]. In our study, a home exercise program was utilized without monitoring instead of supervised physical therapy; therefore, patient compliance might have been low. This might be the reason for the lack of significant changes in the shoulder ROM between the 2- and 4-week follow-up evaluations.
A significant decrease in the SPADI pain and disability sub-scores was also observed in the first 2 weeks. As with the improvement in the ROM, this is also thought to be an effect of HD with corticosteroid injection rather than the home exercises. The minimal clinically important difference (MCID) in the SPADI score generally ranges from 8 to 13 [28]. The average outcomes of the changes in the SPADI score were 31.42 for pain and 22.08 for disability. Therefore, the improvements in the SPADI scores were clinically meaningful because the decreases were greater than the MCID in the study. However, the degree of decline in the SPADI scores was not as much as that reported in a previous study that showed an average decrease of 44.4 for pain and 36.8 for disability at 3 weeks [20]. Therefore, our study suggests that the ROM improvement in the patients with AC after breast cancer surgery was superior to that in the patients with idiopathic AC; however, the effects on the SPADI score did not seem to have improved as much as we expected in the patients with AC after breast cancer surgery. This is because various upper-extremity problems can occur after breast cancer surgery [7,10]. For example, in addition to AC, lymphedema, pectoralis tightness, and myofascial pain syndrome can affect shoulder pain, disability, and QOL among patients.
The distinctive properties of the glenohumeral joint capsules are a higher Pmax at a lower Vmax and stiffer Scap in patients with idiopathic AC than those in healthy individuals among previous studies [13,14]. In this study, the BC group showed a higher Pmax at a similar Vmax and a higher Scap than did the CON group. Because other indicators (Pmax and Vmax) are partially affected by capsule-preserving HD, the Scap is known to be the most accurate parameter of capsular stiffness [15]. Therefore, our study suggests that patients with AC after breast cancer surgery have stiffer capsules than those with idiopathic AC. Factors affecting capsular stiffness can be divided into problems of the capsule itself and those of the surrounding soft tissues, including the ligamentous structures. Postoperative restriction of the shoulder [29], postoperative inflammatory conditions, soft tissue tightness due to radiotherapy [30], and pectoralis tightness [10] are all possible mechanisms that can explain why patients with AC after breast cancer surgery have stiffer capsules than those with idiopathic AC.
In our study, the BCS and RM subgroups showed no significant difference in the biomechanical properties at baseline and all shoulder ROM and SPADI scores at follow-up, except for the ranges of flexion and external rotation and the total ROM at 4 weeks post-HD. At that point, the greater degree of ROM recovery in the BCS group than in the RM group is consistent with the previous finding that the limitation of shoulder ROM was more prominent in patients who underwent mastectomy than in those who underwent BCS [31]. However, these ROM differences resulting from the different types of surgery did not change the pain or disability sub-scores probably because complications other than AC also affect patients [7].
Further studies on this problem are needed to explore the underlying pathophysiological mechanism of AC after breast cancer surgery; the results could be used to establish a finer therapeutic intervention.
This study has several limitations. First, this study was a comparative study of retrospective data for characterizing biomechanical properties. Initially, we attempted to perform propensity score matching. However, owing to the small number of patients who met the inclusion criteria, it was impossible to perform such, resulting in a difference in the mean age. Second, knowing the exact effect of HD with corticosteroid injection is impossible because there was no control group utilized for comparison. However, there have been many previous studies on the effect of HD with corticosteroid treatment on idiopathic AC, and they have reported that HD is one of the most effective methods for managing frozen shoulder [5,6,20–24]. In comparison with these studies, our study found that HD with corticosteroid injection was also effective in treating AC after breast cancer surgery. Nonetheless, the absence of a prospective control group in this study remains a limitation because of the inability to analyze the relationship between shoulder joint capsular stiffness and the treatment progress with HD for AC.
In conclusion, this study demonstrated that HD with corticosteroid injection helped reduce shoulder ROM limitations, pain, and disability in the patients with AC after breast cancer surgery. We also revealed that the stiffness of the glenohumeral joint capsule in the patients who underwent breast cancer surgery and were diagnosed with AC was greater than that in the patients who were diagnosed with idiopathic AC. Further studies are needed to discover the exact pathophysiological mechanisms involved among patients with AC after breast cancer surgery and detailed treatment options for stiffer shoulder capsules.