INTRODUCTION
As Internet network expands, weekly mean time a person spends at a computer has dramatically increased because many people have computers [1]. However, excessive computer use frequently results in musculoskeletal disorder on neck and shoulder [2,3]. The posture of staring at a monitor, located below the height of eyesight, makes the head move forward. Anterior curve in the lower cervical and posterior curve in the upper thoracic vertebrae could be exaggerated [4,5]. This is known as forward head posture or turtle neck syndrome [6,7,8].
A number of people with forward head posture complain of neck problems [9,10,11]. Previous studies reported that abnormal working posture with computer was associated with neck and shoulder pain due to musculoskeletal disorders, especially myofascial pain syndromes (MPS) [12,13]. Prolonged abnormal postures have been regarded as one of the causes of MPS. Therefore, treatment guideline for MPS includes re-education on desirable posture [8,14]. However, few studies have directly evaluated the relationship between forward head posture and MPS in neck and shoulder. The aims of this study were 1) to assess the head posture correctly using cervical spine X-rays and 2) to find out whether abnormal head posture is related to MPS in neck and shoulder.
MATERIALS AND METHODS
Subjects
The study was conducted from January 2006 to March 2009 at the Department of Rehabilitation Medicine, Dankook University Hospital in Korea. Data from patients with posterior neck pain as their main complaints who were diagnosed with MPS were retrospectively extracted from their medical records. MPS was defined as regional muscle tenderness originated from myofascial trigger points [15]. Participants were excluded if they had any of the following conditions: 1) history of cervical trauma or surgery; 2) congenital anomalies involving the spine (cervical, thoracic, and lumbar); 3) bony abnormalities in spine; 4) any disorder of the central or peripheral nervous system; and 5) any systemic arthritis. Age, sex, and symptom duration were recorded. The study protocol was approved by the Institutional Review Board of the Dankook University Hospital (IRB No. DKUH-2014-05-016).
Methods
Radiologic assessments
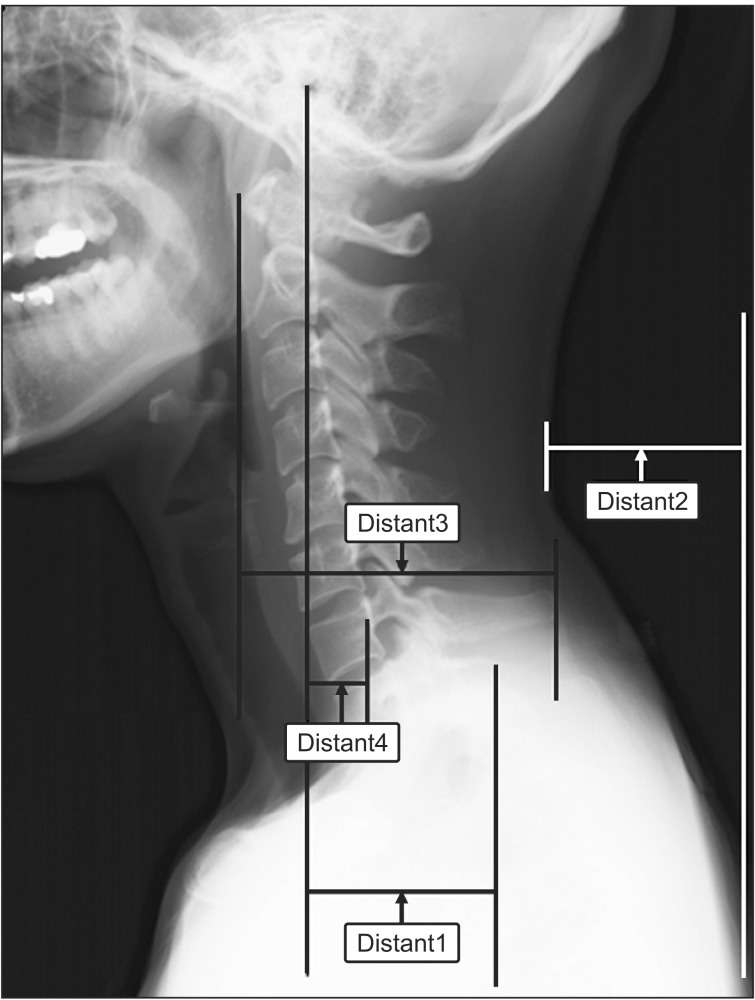
Simple cervical spine X-rays were performed for the study subjects. To take a lateral view of the cervical spine, subjects were sitting in neutral position with head straight. Subjects were asked to elevate their chins straightly and to drop their shoulders as far as possible. The following five parameters were measured in the lateral view of cervical spine X-rays: distant 1 (D1), the horizontal distance between the earhole and lateral shoulder; distant 2 (D2), the horizontal distance between plump line of posterior neck and posterior shoulder; distant 3 (D3), the horizontal distance between the anterior margin of C1 body and the posterior margin of C7 spinous process; distant 4 (D4), the horizontal distance between the earhole and midline of C7 lower margin (Fig. 1); and cervical angle (CA) which was measured on lateral view of cervical spine X-ray from the two tangent lines drawn on the posterior vertebral body margins of C2-C7 (posterior tangent method) [16] (Fig. 2).
Clinical assessments
The presence, location, and number of trigger points in neck and shoulder areas were evaluated for each patient. Scalenus, cervical paraspinal muscle, upper trapezius, levator scapulae, infraspinatus, supraspinatus, rhomboid, teres minor, deltoid, and sternocleidomastoid muscles were examined for myofascial trigger point. The following trigger points were diagnosed using the diagnostic criteria described by Travell and Simons [15]: 1) palpable taut band; 2) spot tenderness in taut band; 3) pain complaint by pressure on the tender nodule; 4) painful limit to full stretch range of motion; 5) visual or tactile local twitch response; and 6) local twitch response induced by needle penetration of tender nodule. Findings from (1) to (4) are essential to the diagnosis. Diagnosis is more certain when criterion (5) or (6) is present.
Statistical analysis
Spearman correlation coefficient was used to investigate the correlation between age, symptom duration, and five parameters. The association between MPS and five parameters were also subjected to Spearman correlation coefficient analysis. All statistical analyses were performed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was considered when p-values were less than 0.05.
RESULTS
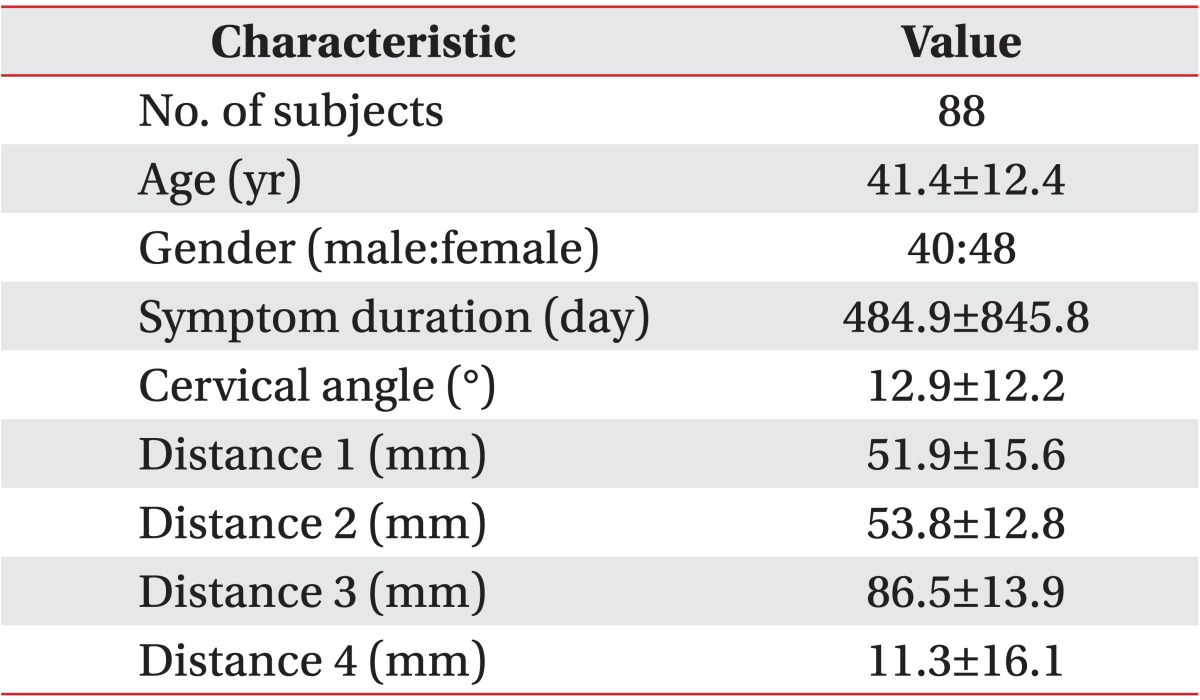
Two hundred and forty-eight persons who visited outpatient clinic with posterior neck pain from January 2006 to March 2009 were screened. Of them, 160 were excluded for the following reasons: history of cervical trauma or surgery (n=45); congenital anomalies involving the spine (n=2); bony abnormalities in spine (n=11); disorder on nervous system diagnosed on electromyography (n=93); and systemic arthritis (n=9). A total of 88 participants (40 men and 48 women) were included in the study. The mean age was 41.4±12.4 years. Symptom duration was 484.9±845.8 days. The demographic data of patients are shown in Table 1.
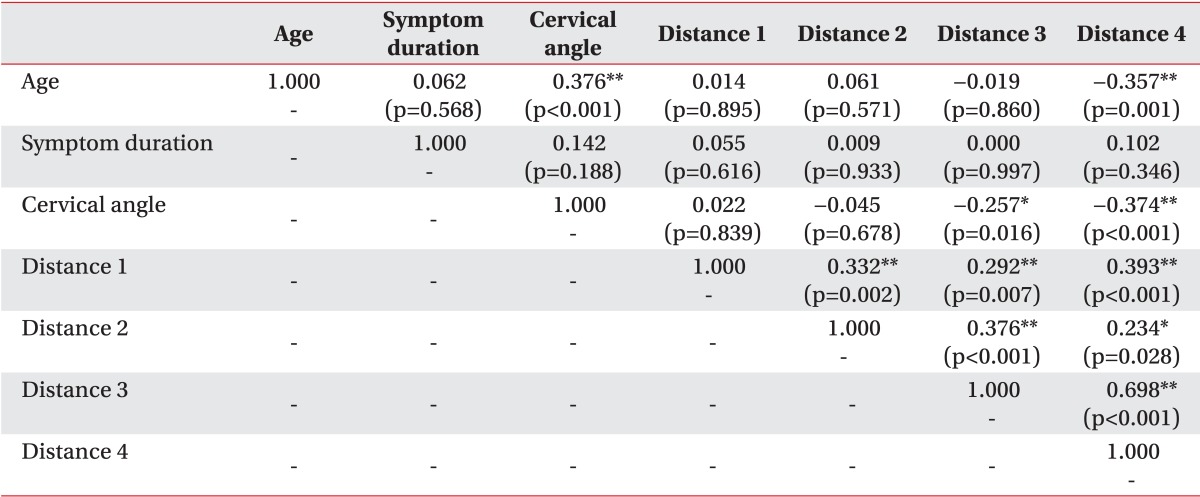
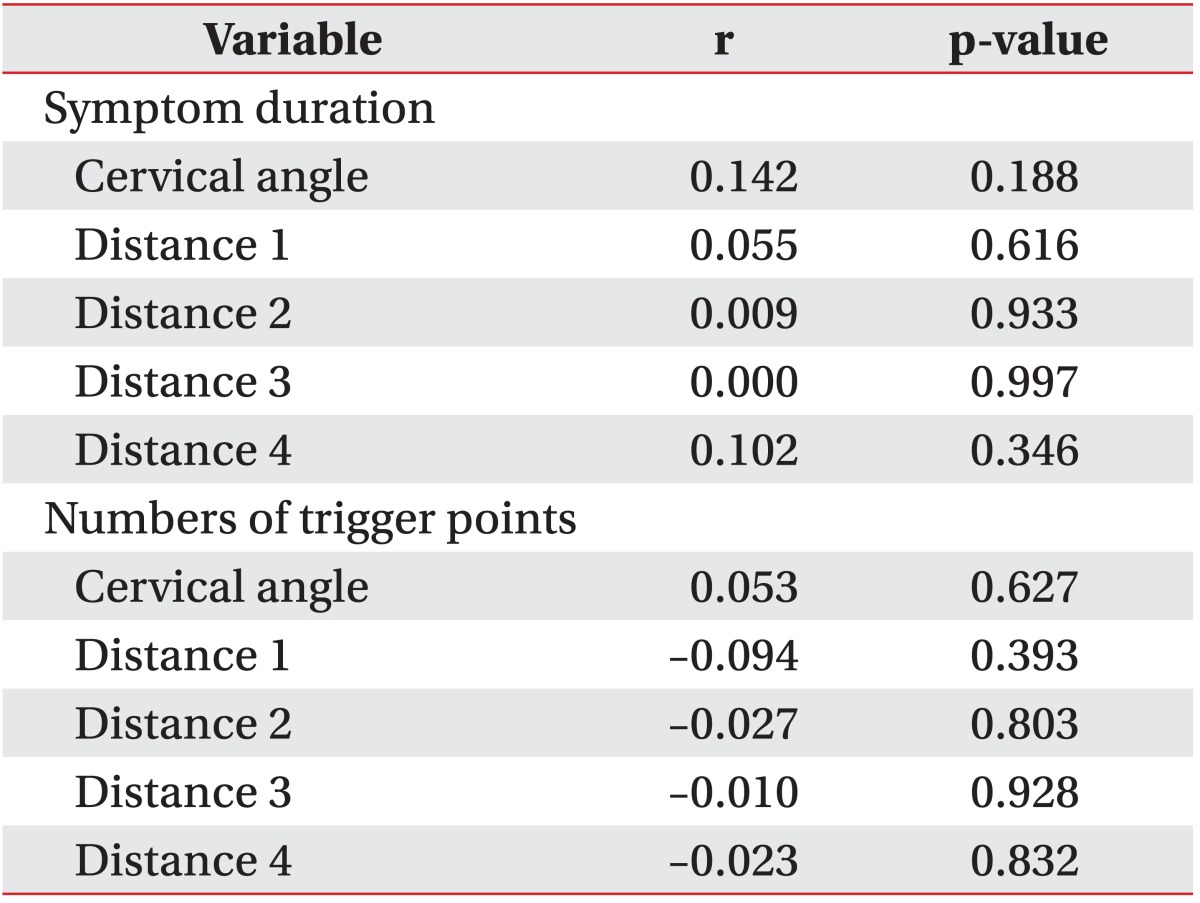
Spearman correlation coefficients among age, symptom duration, CA, D1, D2, D3, and D4 are summarized in Table 2. D3 (the horizontal distances between C1 vertebral body and C7 spinous process) and the D4 (the horizontal distances between the earhole and C7 vertebral body) were negatively correlated with CA, reflecting cervical lordosis (r=-0.257, p=0.016 and r=-0.374, p<0.001, respectively). All distance parameters had positive correlation with each other. Age was positively correlated with CA (r=0.376, p<0.001) but negatively correlated with D4 (r=-0.357, p=0.001). However, the symptom duration did not show significant correlation with any other parameter (Table 2). There were no significant association between the five parameters and the symptom duration of MPS (Table 3). In addition, the numbers of trigger points did not show correlation with the five parameters. The most common location of trigger points was the upper trapezius muscle. The second most common location was the cervical paraspinal muscles. However, there was no relationship between the location of myofascial trigger points and the five parameters.
DISCUSSION
To our knowledge, this study was the first trial to analyze the relationship between forward head posture and MPS. Our results revealed that the greater the forward head position was, the more reduced the cervical lordosis was. This is consistent with a previous report [9]. In addition, according to linear regression analysis, younger patients showed more reduced CA and greater forward head position. In healthy individuals, the degree of forward head posture tends to be increased with age. The trend of this is associated with reduced range of motion in the cervical region [17,18]. However, after comparing the cervical angle of neck pain patients with age-matched pain-free subjects, one study explained that patients who complained spontaneous neck pain may have poorer posture than healthy individuals [11]. Older neck pain patients who have decreased cervical spine mobility due to age-related degenerative change seem to be little affected by poor posture when compared to younger neck pain patients [11]. The results of our study are consistent with the previous study, suggesting that some age-related factors may reduce the changes of cervical spine alignment in posterior neck pain patients. Further studies are needed to clarify this.
There was no relationship between the forward head position and the presence, location, and number of trigger points, suggesting that the mechanism of pain related to the forward head position does not account for myofascial trigger points. Even though mentally challenging computer work is associated with neck pain and forward head posture, only upper trapezius muscle activation was increased. Psychosocial stress with identical cognitive demands may evoke an increase in arousal along with an increase in upper trapezius muscle activity which might consequently lead to neck disturbance [19].
One plausible biomechanical explanation is that the pain associated with forward head position could be originated from the cervical facet joints. There are two mechanism of facet joint pain: excessive compression of the facet joint articulation and the capsular ligament strain beyond the physiologic limit in the forward head posture which stretches anterior structures of the neck and reduces the length of posterior muscles [11,20]. Facet joint compression could damage synovial folds that contain nociceptive nerve endings immunoreactive for substance P and calcitonin gene-related peptide, which could potentially lead to facet pain [21,22]. Because facet joints planes are obliquely oriented, the forward head position might increase the compressive force between the facet articular cartilage of the inferior articular process and the adjacent facet of the superior articular process [23]. The presence of mechanoreceptive and nociceptive nerve endings in cervical facet capsules plays important role in proprioception and pain sensation in the cervical spine [24,25]. Excessive capsular ligaments strain could potentially injure these structures, therefore generating pain [20]. Capsular ligament strain begins during extension but peaks as the facets were returning from maximal extension back to neutral position [20,26]. In patients with forward head position, cervical spine can be considered similar to a protracted position in which the lower cervical vertebrae are flexed in a forward glide with the upper cervical vertebrae extended [1,2,27]. Long standing hyperextensive state of upper cervical vertebrae can cause strain to the upper cervical facet capsular ligament.
Another possible cause is cervical root compression due to decreased cervical foraminal area in the forward head posture. When the forward head posture was corrected especially for lower cervical spine, it would improve the nerve root function by increasing the foraminal volume and area at the foraminal isthmus, which consequently relieves clinical symptoms [10].
There are some limitations of this study. Firstly, during assessment of forward head posture, measurement of CA and distance were disturbed by some technical problems. Forward head posture might be also combined with abnormal posture of shoulder, making it hard to set the fiducial point. In addition, because patients tended to be tense while taking radiographs, it was hard to measure the resting posture. Secondly, there were several difficulties in detecting trigger point. Human neck is covered by numerous layers of cervical muscles in anterior, lateral, and posterior aspects. Consequently, it was hard to distinguish each muscle selectively by manual method. Furthermore, because various factors could influence pain in the forward head posture, it was hard to select the pure effect of abnormal posture on myofascial pain. However, the risks mentioned above would be minimal because a highly trained and specialized medical doctor carefully diagnosed MPS. The measurement of CA and distance were evaluated by one researcher in order to reduce inter-researcher variations.
In conclusion, this study is the first trial to analyze the relationship between forward head posture and MPS assessed by using X-ray measurement. Younger patients with posterior neck pain showed more reduced cervical lordosis with greater forward head position. Reduced cervical lordosis associated with aging was affected by decreased cervical mobility and other factors. However, these abnormalities were not related to the location or the number of trigger points. Further studies are needed to delineate the mechanism of neck pain in patients with forward head posture. Larger controlled studies are needed to confirm the association between head posture and MPS.